
 PDF下载 ( 8687 KB)
PDF下载 ( 8687 KB)

肝部分切除术后低白蛋白血症发生风险机器学习预测模型构建及评价
DOI: 10.12449/JCH260516
Establishment of a predictive model for the risk of hypoalbuminemia after partial hepatectomy based on machine learning methods
-
摘要:
目的 探讨基于术前临床指标构建的机器学习模型在预测肝部分切除术后低白蛋白血症发生风险中的应用价值。 方法 采用回顾性研究方法,收集2018年1月—2023年1月于南方医科大学南方医院行肝部分切除术的857例患者的临床资料,包括人口统计学资料、基础疾病史、肿瘤特征、术前实验室指标和围手术期指标。按7∶3比例将研究数据划分为训练集与测试集。正态分布的计量资料2组间比较采用成组t检验;偏态分布计量资料2组间比较采用两独立样本的Wilcoxon秩和检验;计数资料2组间比较采用χ2检验或Fisher确切概率法。应用最小绝对收缩和选择算子(LASSO)回归筛选特征变量,采用逻辑回归、决策树、人工神经网络、K近邻(KNN)、支持向量机、极度梯度提升和轻量级梯度提升机共7种机器学习算法构建预测模型。采用受试者操作特征曲线下面积(AUC)评估模型区分度,采用DeLong检验比较模型的AUC。采用校准曲线与决策曲线分析评估模型的校准度和临床实用性,并与白蛋白-胆红素(ALBI)评分、终末期肝病模型(MELD)评分进行比较,并利用沙普利加性解释法(SHAP)解释最佳模型的关键影响因素。 结果 最终纳入700例患者,术后发生低白蛋白血症患者283例(40.42%)。LASSO回归筛选出年龄、乙型肝炎、脂肪肝、阻断时间、术前白蛋白(Alb)、手术时长、术中出血量和术前天冬氨酸氨基转移酶(AST)共8个预测因子。在7种机器学习模型中,KNN模型的综合预测效能最优,测试集的AUC为0.835(95%CI:0.781~0.889),敏感度为84.0%,特异度为65.5%。ALBI评分和MELD评分的AUC分别为0.652和0.524,KNN模型的预测效能显著优于上述两项评分(Z值分别为5.309、8.945,P值均<0.001)。校准曲线显示,KNN模型的预测概率与实际发生率一致性良好;决策曲线分析表明,KNN模型在较大阈值范围内具有临床净收益。SHAP分析显示,术前Alb、乙型肝炎、手术时长、年龄为更显著的影响因素,且乙型肝炎与年龄及手术时长存在协同效应。 结论 基于术前临床指标构建的KNN机器学习模型可有效预测肝部分切除术后低白蛋白血症的发生风险,性能优于传统模型,可为临床早期识别高风险患者提供参考依据。 Abstract:Objective To investigate the application value of a machine learning model based on preoperative clinical indicators in predicting the risk of hypoalbuminemia after partial hepatectomy. Methods A retrospective analysis was performed for the clinical data of 700 patients who underwent partial hepatectomy in Nanfang Hospital, Southern Medical University, from January 2018 to January 2023, including demographic data, history of underlying diseases, tumor characteristics, preoperative laboratory markers, and perioperative indicators. The research data were divided into a training set and a test set at a ratio of 7∶3. The two-independent-samples t test was used for comparison of normally distributed continuous data between two groups; the two-independent-samples Wilcoxon rank-sum test was used for comparison of continuous data with skewed distribution between two groups; the chi-square test or the Fisher’s exact test was used for comparison of categorical data between two groups. The least absolute shrinkage and selection operator (LASSO) regression analysis was used to identify characteristic variables, and 7 machine learning algorithms were used to construct predictive models, i.e., logistic regression, decision tree, artificial neural network, K-nearest neighbors (KNN), support vector machine, eXtreme gradient boosting, and light gradient boosting machine. The receiver operating characteristic (ROC) curve and the area under the ROC curve (AUC) were used to assess the discriminatory ability of models, and the DeLong test was used for comparison of AUC. The calibration curve and decision curve analysis were used to assess the calibration and clinical practicability of models, and the models were compared with albumin-bilirubin (ALBI) score and Model for End-Stage Liver Disease (MELD) score. SHapley Additive exPlanations (SHAP) were used to interpret the key influencing factors for the optimal model. Results A total of 700 patients were finally enrolled, 283 (40.42%) developed hypoalbuminemia after surgery. The LASSO regression analysis identified 8 predictive factors of age, hepatitis B, fatty liver, blockade time, preoperative albumin (Alb), time of operation, intraoperative blood loss, and preoperative aspartate aminotransferase (AST). Among the 7 machine learning models, the KNN model showed the best overall predictive performance, with an AUC of 0.835 (95% confidence interval: 0.781 — 0.889), a sensitivity of 84.0%, and a specificity of 65.5% in the test set. ALBI and MELD scores had an AUC of 0.652 and 0.524, respectively, and the KNN model had a better predictive performance than these two scores (Z=5.309 and 8.945, both P <0.001). The calibration curve showed good consistency between predicted probabilities and actual incidence rates, and the decision curve analysis showed that the KNN model had net clinical benefit across a wide threshold range. The SHAP analysis showed that preoperative Alb, hepatitis B, time of operation, and age were the most significant influencing factors, and a synergistic effect was observed between hepatitis B and age/time of operation. Conclusion The KNN machine learning model constructed based on preoperative clinical indicators can effectively predict the risk of hypoalbuminemia after partial hepatectomy and has a better performance than traditional scoring models, which provides a reference for the early identification of high-risk patients in clinical practice. -
Key words:
- Partial Hepatectomy /
- Hypoalbuminemia /
- Machine Learning
-
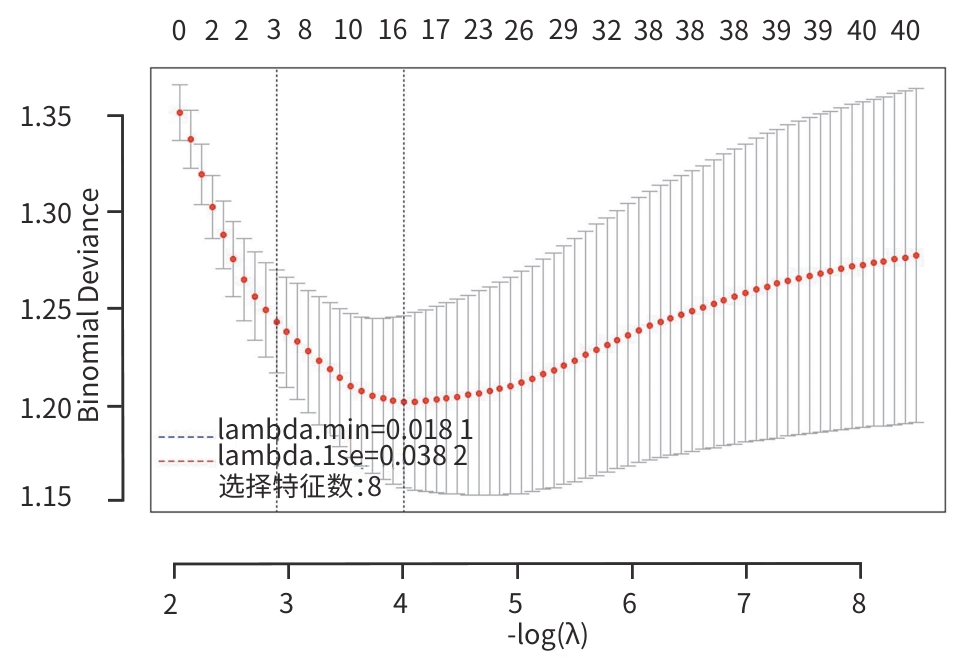
注: LASSO,最小绝对收缩和选择算子。
图 1 LASSO回归变量筛选的10折交叉验证曲线
Figure 1. 10-fold cross-validation curve for variable selection by LASSO regression
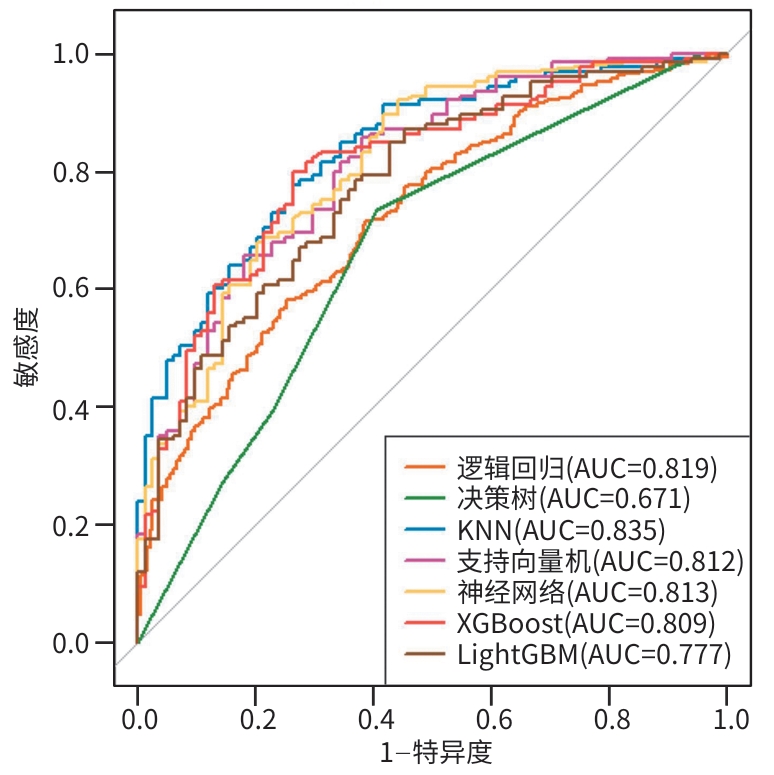
注: ROC曲线,受试者操作特征曲线;KNN,K近邻;XGBoost,极度梯度提升;LightGBM,轻量级梯度提升机;AUC,曲线下面积。
图 2 测试集中不同机器学习模型的ROC曲线
Figure 2. ROC curves of different machine learning models in the test set
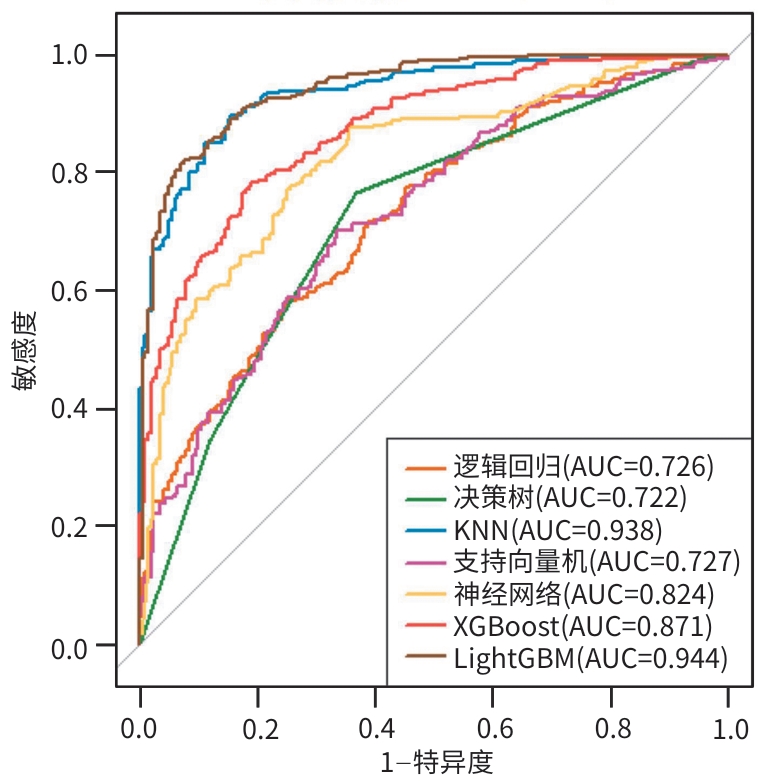
注: ROC曲线,受试者操作特征曲线;KNN,K近邻;XGBoost,极度梯度提升;LightGBM,轻量级梯度提升机;AUC,曲线下面积。
图 3 训练集中不同机器学习模型的ROC曲线
Figure 3. ROC curves of different machine learning models in the training set
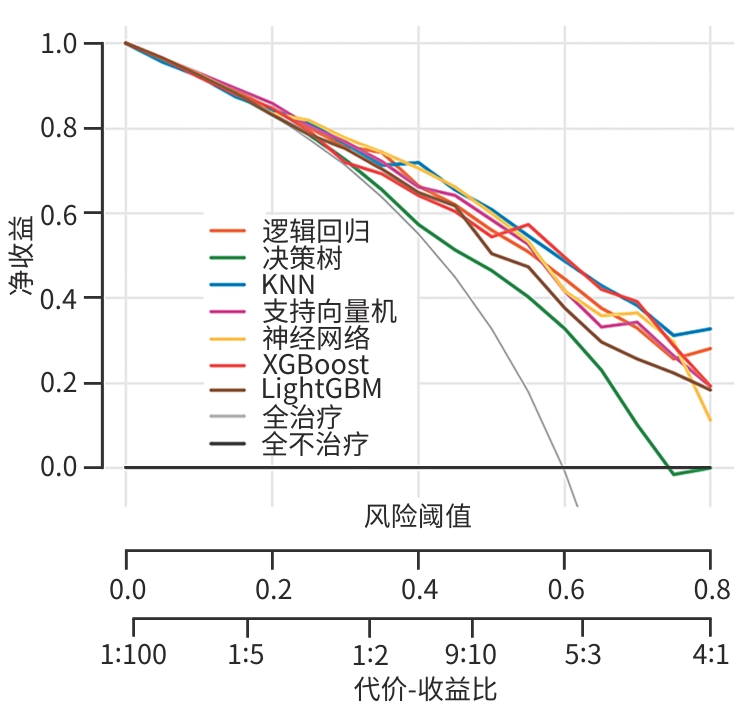
注: KNN,K近邻;XGBoost,极度梯度提升;LightGBM,轻量级梯度提升机。
图 5 各机器学习模型的决策曲线
Figure 5. Decision curves of the machine learning models
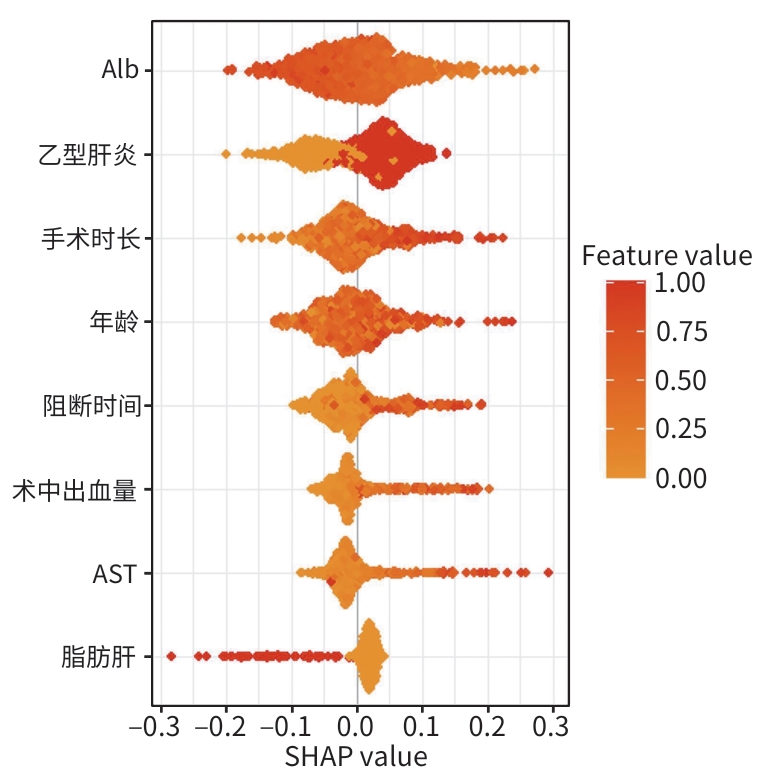
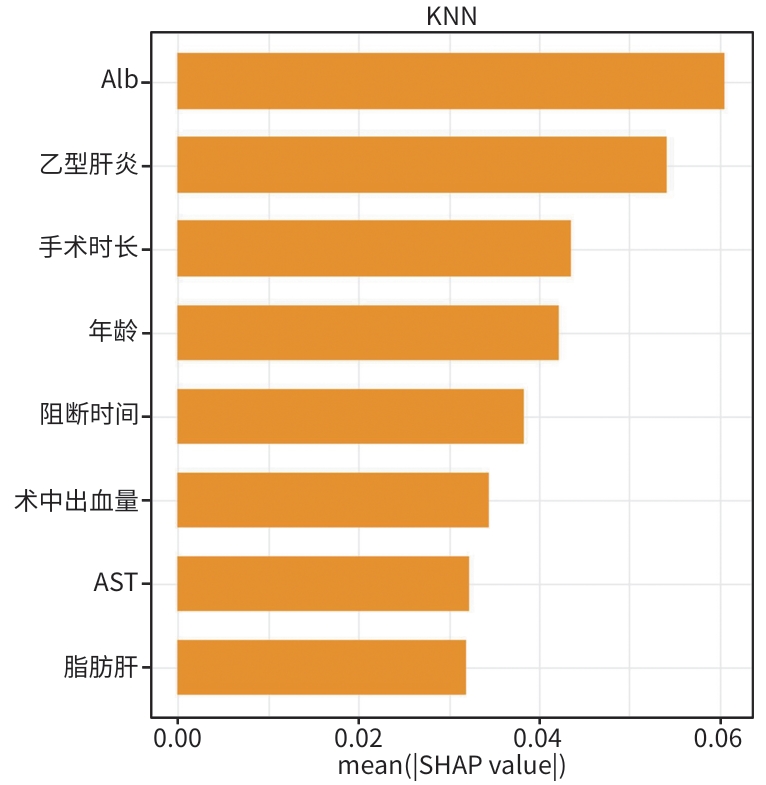
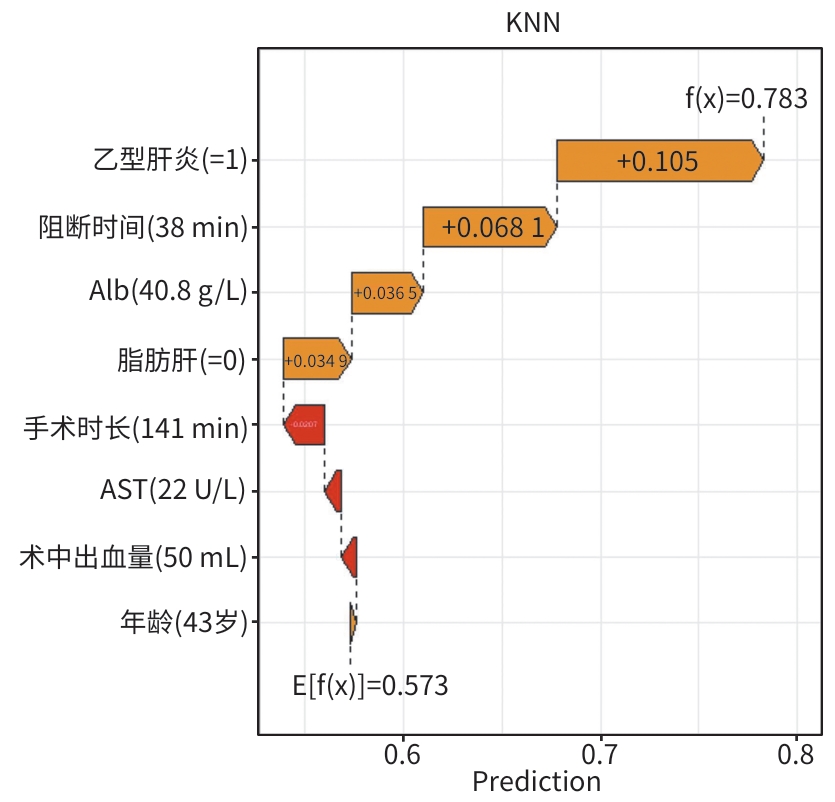
注: Alb,白蛋白;AST,天冬氨酸氨基转移酶;SHAP,沙普利加性解释法。
图 7 K近邻模型预测术后低白蛋白血症的SHAP蜂巢图
Figure 7. Beeswarm plot of SHAP values for the KNN model predicting postoperative hypoalbuminemia
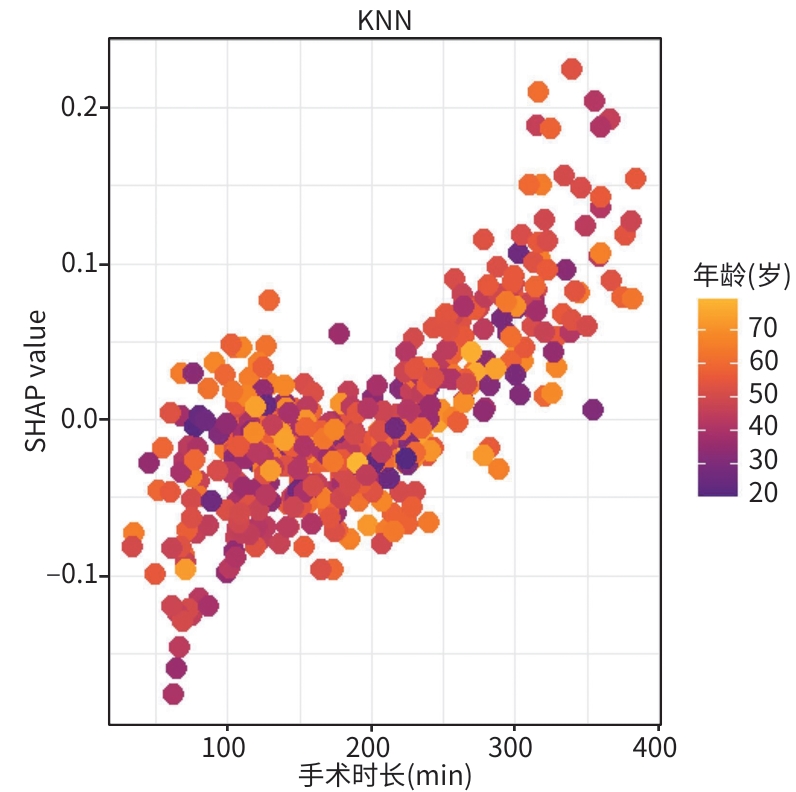
注: KNN,K近邻。
图 8 年龄和手术时长的偏相关依赖图
Figure 8. Partial dependence plot for age and operation duration
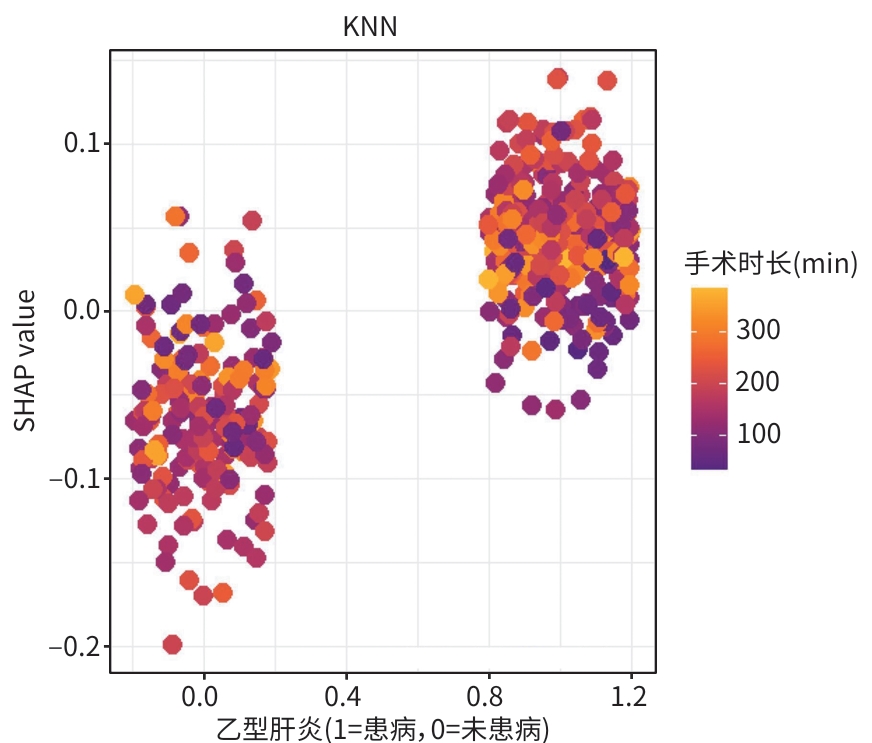
注: KNN,K近邻。
图 9 手术时长和乙型肝炎的偏相关依赖图
Figure 9. Partial dependence plot for operation duration and hepatitis B
表 1 肝部分切除术后患者的基线资料
Table 1. Baseline characteristics of patients after partial hepatectomy
项目 总计(n=700) 低白蛋白组(n=283) 正常组(n=417) 统计值 P值 性别[例(%)] χ2=0.011 0.984 女 184(26.29) 75(26.50) 109(26.14) 男 516(73.71) 208(73.50) 308(73.86) 年龄(岁) 50.9±12.1 48.7±12.3 52.4±11.6 t=4.114 <0.001 体重指数(kg/m2) 23.1±3.2 23.4±3.2 22.9±3.2 t=-1.809 0.071 住院天数(d) 14.3±7.5 13.3±6.1 15.0±8.2 t=2.911 0.002 乙型肝炎[例(%)] 433(61.86) 150(53.00) 283(67.87) χ2=15.783 <0.001 丙型肝炎[例(%)] 20(2.86) 6(2.12) 14(3.36) χ2=0.831 0.464 肝硬化[例(%)] 305(43.57) 103(36.40) 202(48.44) χ2=9.949 0.002 脂肪肝[例(%)] 91(13.00) 48(16.97) 43(10.31) χ2=6.591 0.014 高血压[例(%)] 100(14.29) 41(14.49) 59(14.15) χ2=0.016 0.987 糖尿病[例(%)] 65(9.29) 19(6.71) 46(11.03) χ2=3.731 0.072 门静脉高压[例(%)] 143(20.43) 51(18.02) 92(22.06) χ2=1.694 0.228 门静脉癌栓[例(%)] 15(2.14) 4(1.41) 11(2.64) χ2=1.205 0.405 腹水[例(%)] 28(4.00) 8(2.83) 20(4.80) χ2=1.703 0.268 肝性脑病[例(%)] 1(0.14) 0(0.00) 1(0.24) χ2=0.680 >0.999 术中输血[例(%)] 117(16.71) 33(11.67) 84(20.14) χ2=8.715 0.004 转移[例(%)] 10(1.43) 4(1.41) 6(1.44) χ2=0.001 >0.999 微血管侵犯分级[例(%)] χ2=21.769 <0.001 0级 450(64.29) 209(73.85) 241(57.80) 1级 142(20.29) 36(12.72) 106(25.42) 2级 100(14.29) 36(12.72) 64(15.35) 3级 8(1.14) 2(0.71) 6(1.44) 甲胎蛋白(ng/mL) 5.49(2.20~68.20) 3.70(2.00~33.00) 7.30(2.44~114.00) Z=-3.377 0.050 癌胚抗原(ng/mL) 1.57(0.86~2.45) 1.50(0.82~2.46) 1.58(0.91~2.44) Z=-1.218 0.132 CA19-9(U/mL) 12.63(6.64~20.59) 11.90(6.65~20.61) 13.09(6.63~20.57) Z=-0.323 0.618 肿瘤大小(cm) 5.0±0.3 4.7±0.4 5.2±0.2 t=2.544 0.008 术前凝血酶原时间(s) 11.3±1.1 11.1±1.1 11.4±1.1 t=3.566 <0.001 术前国际标准化比值 1.0±0.4 1.0±0.6 1.0±0.1 t=-0.387 0.747 术前白细胞计数(×109/L) 6.0±0.3 6.2±0.5 5.9±0.2 t=-1.228 0.294 术前淋巴细胞计数(×109/L) 1.77(1.36~2.19) 1.83(1.51~2.22) 1.64(1.24~2.13) Z=-1.548 0.231 术前中性粒细胞计数(×109/L) 3.21(2.48~4.25) 3.16(2.48~4.19) 3.25(2.48~4.27) Z=-0.650 0.287 术前红细胞计数(×1012/L) 4.6±0.7 4.6±0.6 4.6±0.7 t=-0.490 0.612 术前血红蛋白(g/L) 134.3±20.2 136.2±20.6 133.0±19.9 t=-2.034 0.044 术前血小板计数(×109/L) 203.2±86.5 210.8±94.9 198.0±79.9 t=-1.923 0.063 术前丙氨酸氨基转移酶(U/L) 23(15~35) 20(13~30) 25(18~38) Z=-4.216 0.004 术前AST(U/L) 23(17~33) 20(16~27) 25(18~38) Z=-5.784 <0.001 术前总蛋白(g/L) 67.3±5.7 67.5±5.6 67.1±5.8 t=-0.854 0.391 术前Alb(g/L) 39.8±4.2 41.1±4.4 38.9±3.9 t=-6.910 <0.001 术前总胆红素(μmol/L) 13.3±1.6 13.2±1.5 13.3±1.3 t=0.132 0.895 术前直接胆红素(μmol/L) 5.2±0.5 4.9±0.6 5.5±0.4 t=2.245 0.016 术前肌酐(μmol/L) 75.3±19.8 75.5±16.5 75.1±21.7 t=-0.221 0.816 术前钾(mmol/L) 3.96(3.74~4.16) 3.96(3.72~4.16) 3.96(3.75~4.17) Z=-0.283 0.321 术前钠(mmol/L) 140.3±8.6 139.9±11.8 140.6±5.4 t=1.113 0.327 手术时长(min) 196.0±28.0 166.3±24.7 216.2±31.5 t=7.136 <0.001 术中出血量(mL) 100.00(50.00~200.00) 55.87(30.00~150.00) 100.00(50.00~300.00) Z=-5.988 <0.001 阻断时间(min) 9(0~35) 0(0~18) 14(0~42) Z=-4.633 0.005 注:CA19-9,糖类抗原19-9;AST,天冬氨酸氨基转移酶;Alb,白蛋白。
 下载: 导出CSV
下载: 导出CSV
表 2 训练集与测试集基线特征对比
Table 2. Baseline characteristics of training and test sets
变量 训练集(n=491) 测试集(n=209) 统计值 P值 年龄(岁) 51.00±11.80 50.80±12.60 t=0.174 0.862 乙型肝炎[例(%)] χ2=2.245 0.135 否 178(36.25) 89(42.58) 是 313(63.74) 120(57.42) 脂肪肝[例(%)] χ2=0.107 0.744 否 429(87.37) 180(86.12) 是 62(12.63) 29(13.88) 阻断时间(min) 9(0~82) 9(0~71) Z=0.510 0.609 术前Alb(g/L) 39.70±3.97 39.90±3.79 t=0.778 0.438 手术时长(min) 191.37±20.42 187.33±18.56 t=0.593 0.554 术中出血量(mL) 100(5~850) 100(5~800) Z=1.138 0.255 术前AST(U/L) 23(19~93) 21(15~88) Z=0.919 0.358 注:Alb,白蛋白;AST,天冬氨酸氨基转移酶。
下载: 导出CSV
表 3 测试集中不同机器学习模型的性能比较
Table 3. Performance comparison of different machine learning models in the test set
模型 AUC(95%CI) 准确率 特异度 敏感度 阳性预测值 阴性预测值 F1分数 逻辑回归 0.819(0.754~0.872) 0.742 0.631 0.816 0.767 0.697 0.791 KNN 0.835(0.781~0.889) 0.766 0.655 0.840 0.784 0.733 0.811 决策树 0.671(0.598~0.743) 0.679 0.595 0.736 0.736 0.602 0.736 神经网络 0.813(0.754~0.872) 0.766 0.559 0.904 0.753 0.797 0.821 支持向量机 0.812(0.754~0.870) 0.756 0.595 0.864 0.761 0.746 0.809 XGBoost 0.809(0.749~0.868) 0.737 0.571 0.848 0.747 0.716 0.749 LightGBM 0.777(0.714~0.841) 0.713 0.631 0.768 0.756 0.646 0.762 注:KNN,K近邻;XGBoost,极度梯度提升;LightGBM,轻量级梯度提升机;AUC,曲线下面积;95%CI,95%置信区间。
下载: 导出CSV
表 4 训练集中不同机器学习模型的性能比较
Table 4. Performance comparison of different machine learning models in the training set
模型 AUC(95%CI) 准确率 特异度 敏感度 阳性预测值 阴性预测值 F1分数 逻辑回归 0.726(0.682~0.771) 0.682 0.513 0.798 0.706 0.633 0.749 KNN 0.938(0.918~0.958) 0.872 0.789 0.928 0.866 0.882 0.896 决策树 0.722(0.678~0.766) 0.713 0.633 0.767 0.754 0.649 0.760 神经网络 0.824(0.786~0.861) 0.782 0.877 0.643 0.783 0.780 0.706 支持向量机 0.727(0.682~0.772) 0.678 0.462 0.825 0.693 0.643 0.753 XGBoost 0.871(0.841~0.902) 0.786 0.643 0.884 0.784 0.790 0.831 LightGBM 0.944(0.925~0.963) 0.860 0.764 0.925 0.852 0.874 0.887 注:KNN,K近邻;XGBoost,极度梯度提升;LightGBM,轻量级梯度提升机;AUC,曲线下面积;95%CI,95%置信区间。
下载: 导出CSV
-
[1] LIU R, HU SY. Clinical practice guidelines for laparoscopic hepatopancreatobiliary surgery[J]. J Clin Hepatol, 2019, 35( 7): 1450- 1458. DOI: 10.3969/j.issn.1001-5256.2019.07.008.刘荣, 胡三元. 腹腔镜肝胆胰手术操作指南[J]. 临床肝胆病杂志, 2019, 35( 7): 1450- 1458. DOI: 10.3969/j.issn.1001-5256.2019.07.008. [2] GATTA A, VERARDO A, BOLOGNESI M. Hypoalbuminemia[J]. Intern Emerg Med, 2012, 7( 3): 193- 199. DOI: 10.1007/s11739-012-0802-0. [3] LI MX, QIN L, QIU ZC, et al. Influence of platelet-albumin-bilirubin score on textbook outcome of patients with hepatocellular carcinoma after hepatectomy[J]. J Clin Hepatol, 2025, 41( 5): 927- 933. DOI: 10.12449/JCH250519.李梅霞, 覃莉, 邱占成, 等. 血小板-白蛋白-胆红素评分对肝细胞癌患者肝切除术后教科书式结局的影响[J]. 临床肝胆病杂志, 2025, 41( 5): 927- 933. DOI: 10.12449/JCH250519. [4] ROTHSCHILD MA, ORATZ M, SCHREIBER SS. Serum albumin[J]. Hepatology, 1988, 8( 2): 385- 401. DOI: 10.1002/hep.1840080234. [5] FANALI G, di MASI A, TREZZA V, et al. Human serum albumin: From bench to bedside[J]. Mol Aspects Med, 2012, 33( 3): 209- 290. DOI: 10.1016/j.mam.2011.12.002. [6] WEIMANN A, BRAGA M, CARLI F, et al. ESPEN practical guideline: Clinical nutrition in surgery[J]. Clin Nutr, 2021, 40( 7): 4745- 4761. DOI: 10.1016/j.clnu.2021.03.031. [7] SOETERS PB, WOLFE RR, SHENKIN A. Hypoalbuminemia: Pathogenesis and clinical significance[J]. JPEN J Parenter Enteral Nutr, 2019, 43( 2): 181- 193. DOI: 10.1002/jpen.1451. [8] GARCIA-MARTINEZ R, CARACENI P, BERNARDI M, et al. Albumin: Pathophysiologic basis of its role in the treatment of cirrhosis and its complications[J]. Hepatology, 2013, 58( 5): 1836- 1846. DOI: 10.1002/hep.26338. [9] WIEDERMANN CJ. Hypoalbuminemia as surrogate and culprit of infections[J]. Int J Mol Sci, 2021, 22( 9): 4496. DOI: 10.3390/ijms22094496. [10] BOHL DD, SHEN MR, KAYUPOV E, et al. Hypoalbuminemia independently predicts surgical site infection, pneumonia, length of stay, and readmission after total joint arthroplasty[J]. J Arthroplasty, 2016, 31( 1): 15- 21. DOI: 10.1016/j.arth.2015.08.028. [11] BOHL DD, SHEN MR, HANNON CP, et al. Serum albumin predicts survival and postoperative course following surgery for geriatric hip fracture[J]. J Bone Joint Surg Am, 2017, 99( 24): 2110- 2118. DOI: 10.2106/JBJS.16.01620. [12] SHMATKO A, JUNG AW, GAURAV K, et al. Learning the natural history of human disease with generative transformers[J]. Nature, 2025, 647( 8088): 248- 256. DOI: 10.1038/s41586-025-09529-3. [13] CHEN M, DECARY M. Artificial intelligence in healthcare: An essential guide for health leaders[J]. Healthc Manage Forum, 2020, 33( 1): 10- 18. DOI: 10.1177/0840470419873123. [14] PLAUTH M, BERNAL W, DASARATHY S, et al. ESPEN guideline on clinical nutrition in liver disease[J]. Clin Nutr, 2019, 38( 2): 485- 521. DOI: 10.1016/j.clnu.2018.12.022. [15] CHEN GH, JIA WD, YANG Y, et al. Chinese expert consensus on enhanced recovery after hepatectomy(2017)[J]. J Clin Hepatol, 2017, 33( 10): 1876- 1882. DOI: 10.3969/j.issn.1001-5256.2017.10.006.陈规划, 荚卫东, 杨扬, 等. 肝切除术后加速康复中国专家共识(2017版)[J]. 临床肝胆病杂志, 2017, 33( 10): 1876- 1882. DOI: 10.3969/j.issn.1001-5256.2017.10.006. [16] AHN J, SUNDARAM V, AYOUB WS, et al. Hypoalbuminemia is associated with significantly higher liver transplant waitlist mortality and lower probability of receiving liver transplant[J]. J Clin Gastroenterol, 2018, 52( 10): 913- 917. DOI: 10.1097/MCG.0000000000000984. [17] FANG XY, WANG SJ, XU HW, et al. Research progress on the correlation between perioperative hypoalbuminemia and adverse events after spinal surgery[J]. Chin J Spine Spinal Cord, 2025, 35( 1): 91- 95. DOI: 10.3969/j.issn.1004-406X.2025.01.13.房心月, 王善金, 徐浩伟, 等. 围手术期低白蛋白血症与脊柱术后不良事件的相关性研究进展[J]. 中国脊柱脊髓杂志, 2025, 35( 1): 91- 95. DOI: 10.3969/j.issn.1004-406X.2025.01.13. [18] SU ZR, JIA WD, XU GL, et al. Liver functional reserve estimation in hepatitis B virus-related hepatocellular carcinoma: A preliminary study of three methods[J]. Chin J Gen Surg, 2012, 21( 7): 783- 786.苏昭然, 荚卫东, 许戈良, 等. 乙肝相关性肝癌肝脏储备功能评估方案的初步探讨[J]. 中国普通外科杂志, 2012, 21( 7): 783- 786. [19] YU BR, CHEN YW. Basic research on chronic hepatitis B virus infection and metabolic dysfunction: Advances and controversies[J]. J Clin Hepatol, 2024, 40( 3): 446- 452. DOI: 10.12449/JCH240302.余博容, 陈源文. 慢性 HBV 感染与代谢功能障碍基础研究: 当前进展与争议[J]. 临床肝胆病杂志, 2024, 40( 3): 446- 452. DOI: 10.12449/JCH240302. [20] WONG GL, CHAN HL, WONG CK, et al. Liver stiffness-based optimization of hepatocellular carcinoma risk score in patients with chronic hepatitis B[J]. J Hepatol, 2014, 60( 2): 339- 345. DOI: 10.1016/j.jhep.2013.09.029. [21] ALLAN K, GRIMBLE G, WHELAN K, et al. Metabolic response, energy expenditure and nutritional status of patients undergoing coronary artery bypass surgery[J]. Clin Nutr ESPEN, 2025, 68: 869. DOI: 10.1016/j.clnesp.2025.03.155. [22] TØNNESEN E, BACH V, ENGQVIST A, et al. Perioperative electrolyte and fluid management. A survey about knowledge, teaching, routines and placing of responsibility among Danish anaesthetists and surgeons: A-836[J]. Eur J Anaesthesiol, 2004, 21( Supplement 32): 206. DOI: 10.1097/00003643-200406002-00746. [23] HAJIBANDEH S. Comments on“sarcopenia and postoperative complication risk in gastrointestinal surgical oncology: A meta-analysis”[J]. Ann Surg, 2019, 270( 2): e24. DOI: 10.1097/SLA.0000000000003011. [24] QIU JJ, MO XS, TENG YJ, et al. Establishment and evaluation of a nomogram risk prediction model for severe complications in patients after hepatectomy for hepatocellular carcinoma[J]. Chin J Gen Surg, 2021, 30( 1): 24- 31. DOI: 10.7659/j.issn.1005-6947.2021.01.004.邱洁净, 莫新少, 滕艳娟, 等. 肝细胞癌患者肝切除术后严重并发症列线图风险预测模型的建立与评价[J]. 中国普通外科杂志, 2021, 30( 1): 24- 31. DOI: 10.7659/j.issn.1005-6947.2021.01.004. [25] ZHANG SC, ZHOU DC, HOU H, et al. ICG-R15-based clinical prediction model of liver failure after hepatectomy for hepatocellular carcinoma[J]. Acta Univ Med Anhui, 2023, 58( 9): 1593- 1598. DOI: 10.19405/j.cnki.issn1000-1492.2023.09.026.张思成, 周大臣, 侯辉, 等. 基于ICG-R15的肝细胞型肝癌肝切除术后肝衰竭的列线图临床预测模型[J]. 安徽医科大学学报, 2023, 58( 9): 1593- 1598. DOI: 10.19405/j.cnki.issn1000-1492.2023.09.026. [26] JOLIAT GR, KOBAYASHI K, HASEGAWA K, et al. Guidelines for perioperative care for liver surgery: Enhanced recovery after surgery(ERAS) society recommendations 2022[J]. World J Surg, 2023, 47( 1): 11- 34. DOI: 10.1007/s00268-022-06732-5. -

 本文二维码
本文二维码
计量
- 文章访问数: 179
- HTML全文浏览量: 66
- PDF下载量: 81
- 被引次数: 0

