
 PDF下载 ( 4159 KB)
PDF下载 ( 4159 KB)

1990—2023年东亚国家20~44岁青年人群非酒精性脂肪性肝病的疾病负担变化趋势分析
DOI: 10.12449/JCH260509
Changing trend of non-alcoholic fatty liver disease among young people aged 20—44 years in East Asian countries in 1990—2023
-
摘要:
目的 分析1990—2023年东亚国家(中国、朝鲜、日本、蒙古和韩国)青年非酒精性脂肪性肝病(NAFLD)的疾病负担,为制定和调整NAFLD的防治策略提供依据。 方法 基于2023年全球疾病负担(GBD 2023)数据库,提取东亚5国青年NAFLD的发病率、患病率和伤残调整寿命年(DALY)等疾病负担数据,并按国家、性别及年龄分组。使用估计年度百分比变化(EAPC)综合评价1990—2023年青年NAFLD疾病负担的变化趋势,并采用自回归移动平均(ARIMA)模型对中国青年NAFLD疾病负担进行预测。 结果 2023年中国、朝鲜、日本、蒙古和韩国青年NAFLD的标化发病率分别为926.57/10万、805.83/10万、412.66/10万、747.66/10万和534.08/10万;2023年中国、朝鲜、日本、蒙古和韩国青年NAFLD的标化患病率分别为16 817.94/10万、14 500.98/10万、8 534.40/10万、13 705.28/10万和11 587.93/10万;2023年中国、朝鲜、日本、蒙古和韩国青年NAFLD的标化DALY率分别为6.34/10万、10.18/10万、5.23/10万、47.93/10万和6.76/10万。1990—2023年,中国、朝鲜、日本、蒙古和韩国青年NAFLD的标化发病率均呈上升趋势(EAPC:0.87%、0.52%、0.26%、0.48%和0.87%),中国、朝鲜、日本、蒙古和韩国青年NAFLD的标化患病率均呈上升趋势(EAPC:0.99%、0.49%、0.24%、0.59%和0.93%);相反,中国、日本、蒙古和韩国青年NAFLD的标化DALY率均呈下降趋势(EAPC:-2.21%、-2.01%、-0.37%和-4.62%),而朝鲜青年NAFLD的标化DALY率保持相对稳定(EAPC:-0.01%)。性别亚组分析表明,东亚5国青年NAFLD的疾病负担在不同性别中存在明显区别;年龄亚组分析表明,青年NAFLD的发病率随年龄的增长而下降,而青年NAFLD的患病率和DALY率随年龄的增长而上升。此外,未来中国青年NAFLD的标化发病率和标化患病率将进一步上升,而标化DALY率将呈下降趋势。 结论 青年NAFLD的疾病负担在不同国家、性别和年龄段中存在显著差异。未来需进一步结合疾病负担分布特点制定更具针对性的防治措施,从而有效降低青年NAFLD的疾病负担。 Abstract:Objective To investigate the disease burden of non-alcoholic fatty liver disease (NAFLD) among young people in East Asian countries (including China, North Korea, Japan, Mongolia, and South Korea) in 1990—2023, and to provide a basis for formulating and adjusting the prevention and treatment strategies for NAFLD. Methods Related disease burden data of NAFLD among the young people in these five East Asian countries were collected from the Global Burden of Disease 2023 (GBD 2023) database, including incidence rate, prevalence rate, and disability-adjusted life years (DALY), and the young people were divided into groups based on country, sex, and age. Estimated annual percentage change (EAPC) was used to comprehensively evaluate the changing trend of the disease burden of NAFLD among young people from 1990 to 2023, and the Autoregressive Integrated Moving Average model was used to predict the disease burden of NAFLD among the young people in China. Results In 2023, the standardized incidence rates of NAFLD among the young people in China, North Korea, Japan, Mongolia, and South Korea were 926.57/100 000, 805.83/100 000, 412.66/100 000, 747.66/100 000, and 534.08/100 000, respectively; the standardized prevalence rates of NAFLD among the young people in China, North Korea, Japan, Mongolia, and South Korea were 16 817.94/100 000, 14 500.98/100 000, 8 534.40/100 000, 13 705.28/100 000, and 11 587.93/100 000, respectively; the standardized DALY rates of NAFLD among the young people in China, North Korea, Japan, Mongolia, and South Korea were 6.34/100 000, 10.18/100 000, 5.23/100 000, 47.93/100 000, and 6.76/100 000, respectively. From 1990 to 2023, there was a tendency of increase in the standardized incidence rate of NAFLD among the young people in China, North Korea, Japan, Mongolia, and South Korea, with an EAPC of 0.87%, 0.52%, 0.26%, 0.48%, and 0.87%, respectively; there was also a tendency of increase in the standardized prevalence rate of NAFLD among the young people in China, North Korea, Japan, Mongolia, and South Korea, with an EAPC of 0.99%, 0.49%, 0.24%, 0.59%, and 0.93%, respectively; conversely, there was a tendency of reduction in the standardized DALY rate of NAFLD among the young people in China, Japan, Mongolia, and South Korea, with an EAPC of -2.21%, -2.01%, -0.37%, and -4.62%, respectively, while the standardized DALY rate of NAFLD among the young people in North Korea remained relatively stable, with an EAPC of -0.01%. The subgroup analysis based on sex showed that there was a significant difference in the disease burden of NAFLD between the young people with different sexes in the five East Asian countries, and the subgroup analysis based on age showed that the incidence rate of NAFLD in young people decreased with the increase in age, while the prevalence rate and DALY rate of NAFLD increased with age. In addition, the standardized incidence rate and standardized prevalence rate of NAFLD among Chinese young people would further increase in the future, while there would be a reduction in standardized DALY rate in the future. Conclusion There is a significant difference in the disease burden of NAFLD in young people across different countries, sexes, and age groups. In the future, targeted prevention and treatment measures should be developed based on the distribution characteristics of the disease burden of NAFLD, in order to effectively reduce the disease burden of NAFLD among young people. -
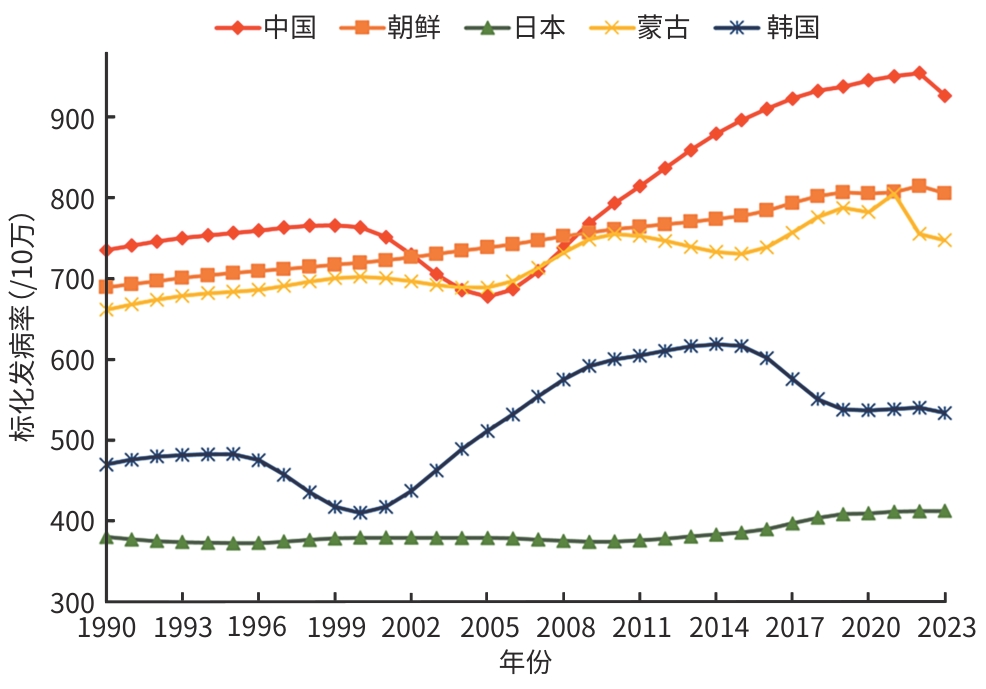
注: NAFLD,非酒精性脂肪性肝病。
图 1 1990—2023年东亚5国青年NAFLD的标化发病率趋势
Figure 1. The standardized incidence trend of NAFLD among youth in the five East Asian countries from 1990 to 2023
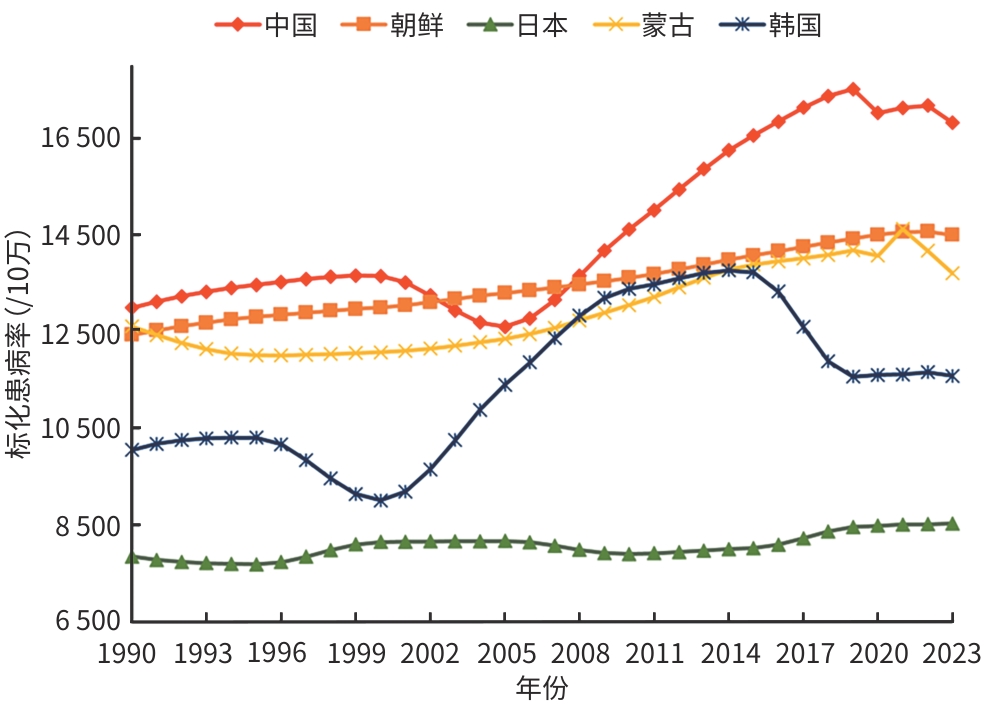
注: NAFLD,非酒精性脂肪性肝病。
图 2 1990—2023年东亚5国青年NAFLD的标化患病率趋势
Figure 2. The standardized prevalence trend of NAFLD among youth in the five East Asian countries from 1990 to 2023
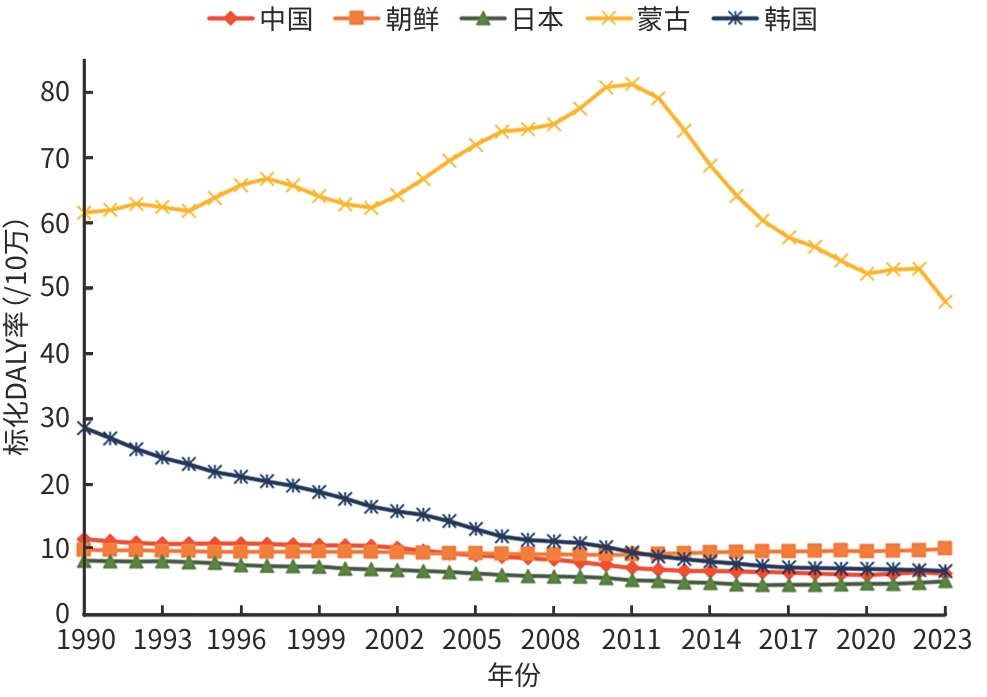
注: NAFLD,非酒精性脂肪性肝病;DALY,伤残调整寿命年。
图 3 1990—2023年东亚5国青年NAFLD的标化DALY率趋势
Figure 3. The standardized DALY rate trend of NAFLD among youth in the five East Asian countries from 1990 to 2023
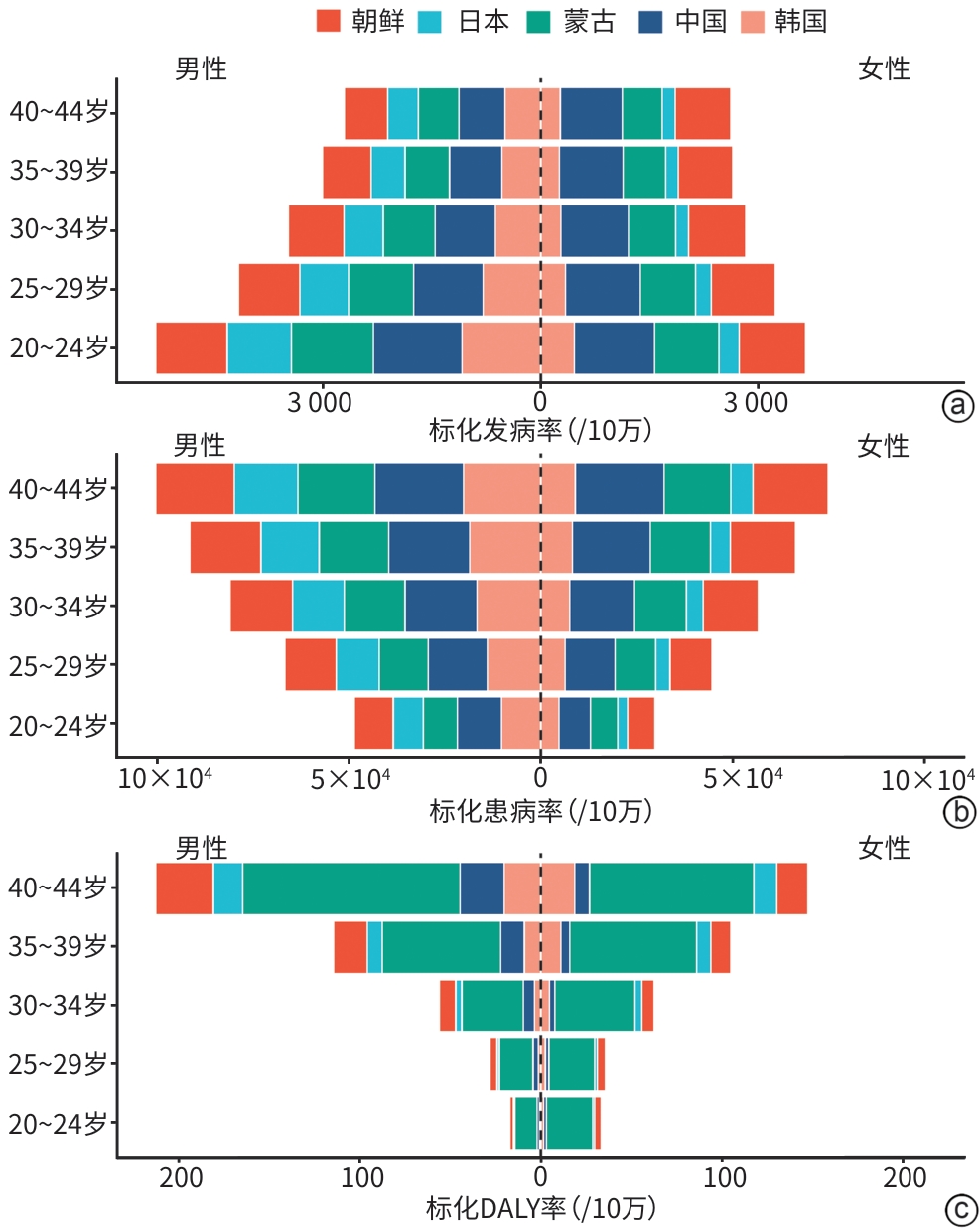
注: a,发病率;b,患病率;c,DALY率。DALY,伤残调整寿命年;NAFLD,非酒精性脂肪性肝病。
图 4 2023年东亚5国青年NAFLD在不同性别和年龄段中的疾病率
Figure 4. Disease rates of NAFLD among young people in the five East Asian countries in 2023, by gender and age group
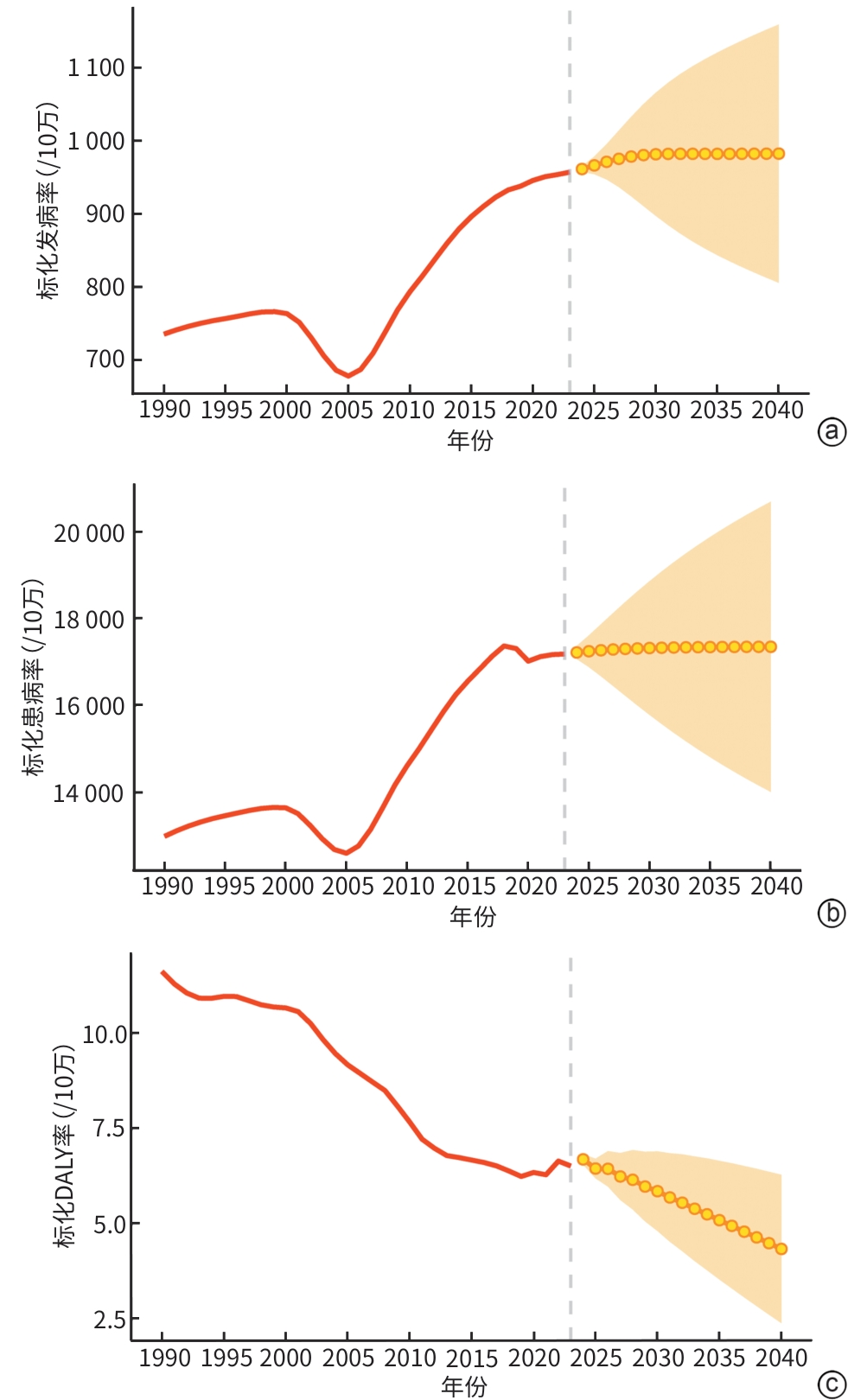
注: a,标化发病率;b,标化患病率;c,标化DALY率。DALY,伤残调整寿命年;NAFLD,非酒精性脂肪性肝病。
图 5 中国青年NAFLD负担的未来预测
Figure 5. Future prediction of the burden of NAFLD among Chinese youth
表 1 1990年和2023年东亚5国青年NAFLD的发病率负担
Table 1. Incidence burden of NAFLD among youth in five East Asian countries in 1990 and 2023
项目 1990年发病数
(例)(95%UI)1990年标化发病率
(/10万)(95%UI)2023年发病数
(例)(95%UI)2023年标化发病率
(/10万)(95%UI)标化发病率EAPC
(%)(95%CI)中国 总体 3 678 695
(2 615 335~4 941 148)735.54
(519.09~994.53)4 159 218
(2 867 628~5 702 460)926.57
(644.10~1 253.90)0.87(0.63~1.11) 男性 1 853 374
(1 295 300~2 509 901)712.04
(494.79~969.90)2 065 632
(1 422 355~2 833 679)889.30
(617.62~1 207.52)1.08(0.71~1.44) 女性 1 825 321
(1 282 271~2 444 003)761.45
(531.91~1 025.96)2 093 586
(1 437 876~2 869 080)965.96
(669.75~1 307.83)0.65(0.46~0.83) 朝鲜 总体 55 542
(38 980~75 114)689.36
(481.20~937.27)80 142
(55 842~108 282)805.83
(562.83~1 085.89)0.52(0.50~0.54) 男性 27 540
(18 943~37 647)665.64
(455.67~916.66)39 184
(26 669~53 744)784.54
(534.41~1 074.02)0.53(0.51~0.55) 女性 28 002
(19 462~37 990)712.14
(493.01~970.31)40 958
(28 248~56 057)826.19
(571.91~1 126.72)0.51(0.49~0.52) 日本 总体 164 171
(115 525~221 883)380.72
(268.92~512.18)132 213
(92 461~180 206)412.66
(290.44~558.10)0.26(0.19~0.34) 男性 122 491
(86 647~165 194)564.43
(400.42~757.07)99 070
(69 415~134 364)609.59
(429.88~819.86)0.22(0.13~0.30) 女性 41 680
(28 360~58 091)192.65
(131.45~268.12)33 143
(22 111~47 364)207.78
(139.43~295.18)0.37(0.12~0.63) 蒙古 总体 5 030
(3 546~6 793)661.87
(463.57~902.65)9 187
(6 379~12 517)747.66
(522.04~1 012.79)0.48(0.41~0.56) 男性 2 692
(1 877~3 608)706.47
(488.95~956.78)4 894
(3 390~6 616)798.39
(555.23~1 073.48)0.40(0.33~0.47) 女性 2 339
(1 596~3 242)617.67
(419.69~863.70)4 293
(2 898~6 010)696.36
(472.11~970.01)0.57(0.45~0.69) 韩国 总体 92 308
(63 433~126 245)470.15
(321.83~645.64)87 917
(60 138~122 765)534.08
(368.53~738.63)0.87(0.54~1.21) 男性 64 495
(44 244~88 682)638.85
(436.82~882.33)62 125
(42 492~86 392)721.82
(497.98~993.55)0.87(0.48~1.27) 女性 27 813
(18 031~39 779)292.48
(189.03~419.59)25 792
(16 570~37 036)326.59
(211.28~465.67)0.72(0.48~0.96) 注:NAFLD,非酒精性脂肪性肝病;EAPC,估计年度百分比变化;95%UI,95%不确定区间;95%CI,95%置信区间。
 下载: 导出CSV
下载: 导出CSV
表 2 1990年和2023年东亚5国青年NAFLD的患病率负担
Table 2. Prevalence burden of NAFLD among youth in five East Asian countries in 1990 and 2023
项目 1990年患病数
(例)(95%UI)1990年标化患病率
(/10万)(95%UI)2023年患病数
(例)(95%UI)2023年标化患病率
(/10万)(95%UI)标化患病率
EAPC(%)
(95%CI)中国 总体 61 184 354
(51 556 516~71 829 460)12 993.77
(10 972.92~15 224.28)82 851 540
(70 037 189~96 825 591)16 817.94
(14 203.26~19 706.30)0.99(0.78~1.20) 男性 33 533 773
(28 354 178~39 309 580)13 671.11
(11 585.18~15 994.99)44 932 931
(37 973 334~52 690 958)17 645.77
(14 880.16~20 732.88)1.22(0.92~1.53) 女性 27 650 581
(23 240 198~32 588 535)12 275.46
(10 337.45~14 450.79)37 918 609
(31 797 776~44 454 123)15 883.07
(13 302.09~18 650.44)0.71(0.53~0.89) 朝鲜 总体 946 694
(800 304~1 115 346)12 437.51
(10 539.79~14 625.90)1 483 738
(1 264 436~1 737 763)14 500.98
(12 341.96~16 994.96)0.49(0.47~0.51) 男性 509 116
(425 303~605 730)13 177.54
(11 036.20~15 640.19)792 313
(670 408~937 410)15 519.75
(13 121.28~18 374.96)0.51(0.49~0.54) 女性 437 578
(364 428~520 351)11 659.92
(9 726.96~13 850.31)691 425
(579 686~817 333)13 457.06
(11 267.61~15 919.37)0.47(0.45~0.49) 日本 总体 3 606 495
(3 109 469~4 172 396)7 852.43
(6 756.82~9 100.87)2 962 204
(2 557 744~3 434 705)8 534.40
(7 350.15~9 922.01)0.24(0.17~0.31) 男性 2 706 182v(2 332 727~3 114 368) 11 694.64v(10 056.53~13 484.42) 2 230 888
(1 923 603~2 571 218)12 633.44
(10 859.73~14 602.43)0.18(0.05~0.30) 女性 900 313
(747 822~1 074 336)3 938.76
(3 274.48~4 702.24)731 316
(597 356~897 006)4 278.33
(3 492.83~5 253.26)0.41(0.19~0.62) 蒙古 总体 84 441
(70 000~100 463)12 608.94
(10 504.54~14 939.53)178 380
(150 803~209 785)13 705.28
(11 557.33~16 151.10)0.59(0.49~0.69) 男性 44 593
(36 884~53 086)13 314.42
(11 062.68~15 786.30)96 411
(81 343~113 273)14 834.78
(12 495.19~17 457.13)0.53(0.44~0.62) 女性 39 848
(31 751~48 583)11 904.39
(9 510.54~14 464.96)81 969
(66 594~99 480)12 573.89
(10 197.61~15 287.92)0.65(0.49~0.80) 韩国 总体 1 891 494
(1 592 056~2 219 372)10 052.89
(8 474.72~11 778.81)2 090 778
(1 758 488~2 459 918)11 587.93
(9 715.85~13 658.71)0.93(0.57~1.29) 男性 1 312 776
(1 106 237~1 542 562)13 621.66
(11 504.15~15 986.57)1 489 301
(1 257 652~1 750 550)15 648.93
(13 167.77~18 445.48)0.95(0.53~1.37) 女性 578 717
(451 098~724 537)6 297.71
(4 918.80~7 871.85)601 478
(470 334~757 444)7 058.26
(5 504.93~8 905.37)0.76(0.50~1.03) 注:NAFLD,非酒精性脂肪性肝病;EAPC,估计年度百分比变化;95%UI,95%不确定区间;95%CI,95%置信区间。
下载: 导出CSV
表 3 1990—2023年东亚5国青年NAFLD的DALY负担
Table 3. DALY burden of NAFLD among youth in five East Asian countries in 1990 and 2023
项目 1990年DALY
(人年)(95%UI)1990年标化DALY
率(/10万)(95%UI)2023年DALY
(人年)(95%UI)2023年标化DALY率
(/10万)(95%UI)标化DALY率EAPC
(%)(95%CI)中国 总体 51 925(36 108~75 488) 11.64(8.10~16.89) 33 563(22 814~47 384) 6.34(4.31~8.95) -2.21(-2.41~-2.02) 男性 29 327(18 298~46 648) 12.79(8.00~20.28) 24 410(15 237~36 003) 8.82(5.49~13.02) -1.43(-1.69~-1.18) 女性 22 598(15 377~32 603) 10.39(7.08~14.95) 9 153(6 115~13 547) 3.70(2.47~5.47) -3.57(-3.74~-3.41) 朝鲜 总体 716(382~1 202) 9.98(5.33~16.69) 1 067(517~1 822) 10.18(4.94~17.40) -0.01(-0.10~0.07) 男性 491(240~875) 13.89(6.84~24.68) 636(287~1 147) 12.20(5.50~22.00) -0.48(-0.59~-0.37) 女性 225(113~378) 6.16(3.10~10.27) 430(198~821) 8.25(3.79~15.73) 0.82(0.77~0.88) 日本 总体 4 376(2 825~6 770) 8.35(5.35~12.97) 2 054(1 289~3 229) 5.23(3.27~8.26) -2.01(-2.19~-1.83) 男性 2 984(1 947~4 600) 11.16(7.24~17.26) 1 103(678~1 786) 5.46(3.35~8.86) -2.97(-3.21~-2.72) 女性 1 391(849~2 217) 5.50(3.32~8.83) 951(568~1 507) 4.99(2.98~7.93) -0.57(-0.72~-0.41) 蒙古 总体 380(221~598) 61.59(35.93~96.00) 638(381~986) 47.93(28.64~74.24) -0.37(-0.82~0.09) 男性 108(57~186) 35.11(18.49~60.68) 313(171~524) 46.85(25.67~78.47) 1.25(0.60~1.91) 女性 272(146~451) 88.19(47.54~144.02) 325(178~526) 49.08(26.72~79.65) -1.44(-1.82~-1.06) 韩国 总体 4 923(2 856~7 938) 28.63(16.69~45.94) 1 395(821~2 210) 6.76(3.94~10.79) -4.62(-4.82~-4.42) 男性 3 327(1 900~5 421) 37.90(21.80~61.54) 706(398~1 134) 6.40(3.57~10.35) -5.97(-6.20~-5.74) 女性 1 597(892~2 588) 18.75(10.50~30.27) 688(380~1 161) 7.18(3.92~12.19) -2.55(-2.83~-2.27) 注:NAFLD,非酒精性脂肪性肝病;EAPC,估计年度百分比变化;95%UI,95%不确定区间;95%CI,95%置信区间。
下载: 导出CSV
-
[1] TANG J, ZHENG N, YAN YX, et al. 1990-2021 global, regional, and national analysis of the burden and trends of non-alcoholic fatty liver disease[J]. Front Med, 2025, 12: 1609816. DOI: 10.3389/fmed.2025.1609816. [2] ZHAO XY, XU D, JI W, et al. Global and Chinese burden of non-alcoholic fatty liver disease in chronic liver disease: Findings from the Global Burden of Disease Study 2021[J]. Chin Med J, 2025, 138( 14): 1741- 1751. DOI: 10.1097/CM9.0000000000003726. [3] HAO XY, SONG H, SU X, et al. Prophylactic effects of nutrition, dietary strategies, exercise, lifestyle and environment on nonalcoholic fatty liver disease[J]. Ann Med, 2025, 57( 1): 2464223. DOI: 10.1080/07853890.2025.2464223. [4] ALALWANI J, ELJAZZAR S, BASIL M, et al. The impact of health status, diet and lifestyle on non-alcoholic fatty liver disease: Narrative review[J]. Clin Obes, 2022, 12( 4): e12525. DOI: 10.1111/cob.12525. [5] LIU CL, ZHU SJ, ZHANG J, et al. Global, regional, and national burden of liver cancer due to non-alcoholic steatohepatitis, 1990-2019: A decomposition and age-period-cohort analysis[J]. J Gastroenterol, 2023, 58( 12): 1222- 1236. DOI: 10.1007/s00535-023-02040-4. [6] GU Y, GUO CN, LIU ZQ, et al. The trend in incidence of non-alcoholic fatty liver disease and its impact on cirrhosis and liver cancer: An analysis from Global Burden of Disease 2021[J]. Public Health, 2025, 242: 79- 86. DOI: 10.1016/j.puhe.2025.02.028. [7] YEUNG SL AU, BORGES MC, WONG THT, et al. Evaluating the role of non-alcoholic fatty liver disease in cardiovascular diseases and type 2 diabetes: A Mendelian randomization study in Europeans and East Asians[J]. Int J Epidemiol, 2023, 52( 3): 921- 931. DOI: 10.1093/ije/dyac212. [8] GAO YQ, YAO JJ, LIU SY, et al. Association between metabolic-associated fatty liver disease and risk of cardiometabolic multimorbidity: A disease trajectory analysis in UK Biobank[J]. Front Endocrinol, 2025, 16: 1585725. DOI: 10.3389/fendo.2025.1585725. [9] SI HAY, ONG KL, SANTOMAURO DF, et al. Burden of 375 diseases and injuries, risk-attributable burden of 88 risk factors, and healthy life expectancy in 204 countries and territories, including 660 subnational locations, 1990-2023: A systematic analysis for the Global Burden of Disease Study 2023[J]. Lancet, 2025, 406( 10513): 1873- 1922. DOI: 10.1016/S0140-6736(25)01637-X. [10] WU JX, DENG YP, TONG KL, et al. Incidence and prevalence of dysthymia among young adults in China, 1990-2021, with forecasts to 2046: An age-period-cohort analysis of the Global Burden of Disease Study 2021[J]. BMC Psychiatry, 2025, 25( 1): 238. DOI: 10.1186/s12888-025-06680-z. [11] LOU JQ, XIANG ZY, ZHU XY, et al. Trends and levels of the global, regional, and national burden of injuries from 1990 to 2021: Findings from the global burden of disease study 2021[J]. Ann Med, 2025, 57( 1): 2537917. DOI: 10.1080/07853890.2025.2537917. [12] XU K, QIAN WL, XU WJ, et al. Global, regional, and national epidemiology of childhood epilepsy from 1990 to 2021: A systematic study based on the GBD 2021[J]. Seizure, 2025, 131: 351- 360. DOI: 10.1016/j.seizure.2025.08.001. [13] HU QG, HAN KX, SHEN JP, et al. Association of weight-adjusted-waist index with non-alcoholic fatty liver disease and liver fibrosis: A cross-sectional study based on NHANES[J]. Eur J Med Res, 2023, 28( 1): 263. DOI: 10.1186/s40001-023-01205-4. [14] ZENG JJ, GU CH, WEN CL, et al. The burden of NAFLD(now referred to as MASLD)-related chronic liver disease and cirrhosis from 1990 to 2021 with projections to 2036: A comparative study of global China the United States and India[J]. Lipids Health Dis, 2025, 24( 1): 298. DOI: 10.1186/s12944-025-02750-z. [15] CHEN YF, WANG GY, HOU ZY, et al. Comparative diabetes mellitus burden trends across global, Chinese, US, and Indian populations using GBD 2021 database[J]. Sci Rep, 2025, 15( 1): 11955. DOI: 10.1038/s41598-025-96175-4. [16] YANG N, LIU TJ, LONG HY, et al. Global burden of male smoking-induced stroke, 1990-2021, and 20-year projections: An analysis of the 2021 Global Burden of Disease Study[J]. BMC Public Health, 2025, 25( 1): 2694. DOI: 10.1186/s12889-025-24021-3. [17] VANCELLS LUJAN P, VIÑAS ESMEL E, SACANELLA MESEGUER E. Overview of non-alcoholic fatty liver disease(NAFLD) and the role of sugary food consumption and other dietary components in its development[J]. Nutrients, 2021, 13( 5): 1442. DOI: 10.3390/nu13051442. [18] TROVATO FM, MARTINES GF, BRISCHETTO D, et al. Fatty liver disease and lifestyle in youngsters: Diet, food intake frequency, exercise, sleep shortage and fashion[J]. Liver Int, 2016, 36( 3): 427- 433. DOI: 10.1111/liv.12957. [19] ZHU ZX, ZHU WM, ZHOU HY, et al. Association between exposure to air pollutants and NAFLD/MAFLD: A meta-analysis[J]. BMC Public Health, 2025, 25( 1): 2672. DOI: 10.1186/s12889-025-24058-4. [20] LI YP, JI H, TIAN F, et al. Association between cumulative uric acid exposure and metabolic dysfunction-associated fatty liver disease[J]. BMC Gastroenterol, 2025, 25( 1): 497. DOI: 10.1186/s12876-025-04038-z. [21] SALMANIZADEH F, SABZEVARI S, SHAFIEIPOUR S, et al. Challenges and needs in the management of non-alcoholic fatty liver disease from the perspective of gastroenterology and hepatology specialists: A qualitative study[J]. BMC Gastroenterol, 2025, 25( 1): 396. DOI: 10.1186/s12876-025-03921-z. [22] WU XG, ZHANG T, PARK S. Dietary quality, perceived health, and psychological status as key risk factors for newly developed metabolic dysfunction-associated steatotic liver disease in a longitudinal study[J]. Nutrition, 2025, 130: 112604. DOI: 10.1016/j.nut.2024.112604. -

 本文二维码
本文二维码
计量
- 文章访问数: 196
- HTML全文浏览量: 51
- PDF下载量: 77
- 被引次数: 0

