
 PDF下载 ( 2849 KB)
PDF下载 ( 2849 KB)

聚乙二醇干扰素α-2b治疗低水平乙型肝炎表面抗原慢性乙型肝炎临床治愈列线图模型的构建
DOI: 10.12449/JCH260508
Construction of a nomogram model for clinical cure of chronic hepatitis B with a low level of hepatitis B surface antigen treated with pegylated interferon α-2b
-
摘要:
目的 筛选聚乙二醇干扰素α-2b(PEG-IFN-α-2b)治疗乙型肝炎表面抗原(HBsAg)低水平慢性乙型肝炎(CHB)患者实现HBsAg清除的相关预测因素,构建基于多因素的联合预测模型并绘制列线图,为临床个体化治疗方案制定及疗效预判提供参考依据。 方法 回顾性分析2022年1月—2024年1月于昆明市第三人民医院就诊并接受PEG-IFN-α-2b治疗的HBsAg<1 500 IU/mL的167例CHB患者,根据其是否实现临床治愈将患者分为HBsAg清除组和HBsAg未清除组。收集患者一般资料和治疗中不同时间节点的血清学生化指标、病毒学指标。符合正态分布的计量资料采用独立样本t检验;非正态分布的计量资料采用Mann-Whitney U检验;计数资料比较采用χ2检验。多因素Logistic回归分析独立影响因素。受试者操作特征(ROC)曲线分析单个指标以及联合预测因子对评估临床治愈的诊断价值,绘制校准曲线,对风险预测模型进行评价。 结果 单因素分析显示,两组患者的年龄(t=-6.839)、核苷(酸)类似物(NA)治疗史1年以上(χ2=59.339)、基因分型(χ2=4.610)、非酒精性脂肪性肝病(χ2=5.319)、治疗前乙型肝炎病毒DNA状态(χ2=60.861)、代偿期肝硬化(χ2=10.960)、治疗前乙型肝炎e抗原(HBeAg)状态(χ2=19.060)、有IFN治疗史(χ2=8.162)、治疗后出现IFN抗体(χ2=12.858)、治疗前HBsAg水平(Z=-7.412)、基线丙氨酸氨基转移酶(ALT)水平(Z=-6.117)、治疗12周ALT水平(Z=-7.171)、治疗24周血小板(PLT)水平(Z=-3.622)、治疗24周促甲状腺激素(TSH)水平(Z=-2.830)比较,差异均有统计学意义(P值均<0.05)。多因素Logistic回归分析显示,年龄[比值比(OR)=1.230,P=0.007]、NA治疗史1年以上(OR=0.008,P=0.011)、治疗前HBeAg状态(OR=0.003,P=0.012)、治疗前HBsAg水平(OR=1.005,P=0.014)、基线ALT水平(OR=0.949,P=0.014)、治疗12周ALT水平(OR=0.969,P=0.016)、治疗24周PLT水平(OR=0.969,P=0.022)、治疗24周TSH水平(OR=3.608,P=0.045)是HBsAg<1 500 IU/mL的CHB患者治疗48周实现HBsAg清除的独立影响因素。Hosmer-Lemeshow拟合优度检验显示χ2=1.398,P=0.994,提示模型拟合良好。用Bootstrap法对列线图模型进行内部验证,校准曲线与理想曲线拟合良好,校准曲线平均绝对误差为0.029。ROC曲线分析显示,联合预测因子的曲线下面积为0.982(95%CI:0.961~0.999),敏感度为94.10%,特异度为93.10%,提示列线图模型具有较好的区分能力。进一步分析显示,不同特征下HBsAg<1 500 IU/mL的CHB患者治疗48周的HBsAg清除率比较,治疗前HBsAg水平≤67.65 IU/mL时,HBsAg清除率为69.60%;基线ALT水平≥62.50 U/L时,HBsAg清除率为58.30%;治疗12周ALT水平≥92.50 U/L时,HBsAg清除率为68.30%;治疗24周PLT水平≥104×109/L时,HBsAg清除率为42.40%;治疗24周TSH水平≤1.38 μIU/mL时,HBsAg清除率为48.30%,两组间比较差异均有统计学意义(P值均<0.001)。 结论 年龄、NA治疗史1年以上、治疗前HBeAg状态、治疗前HBsAg水平、基线ALT水平、治疗12周ALT水平、治疗24周PLT水平和治疗24周TSH水平为独立预测因素,所构建的联合预测列线图模型对PEG-IFN-α-2b治疗HBsAg<1 500 IU/mL的CHB患者治疗48周实现临床治愈具有较高的预测价值,可为筛选适合治疗人群和预测临床治愈提供参考。 Abstract:Objective To investigate the predictive factors for HBsAg clearance in chronic hepatitis B (CHB) patients with a low level of hepatitis B surface antigen (HBsAg) treated with pegylated interferon α-2b (PEG-IFN-α-2b), to establish a combined predictive model and a nomogram based on multiple factors, and to provide a reference for formulating individualized treatment regimens and predicting treatment outcome in clinical practice. Methods A retrospective analysis was performed for 167 CHB patients with HBsAg <1 500 IU/mL who attended The Third People’s Hospital of Kunming from January 2022 to January 2024 and were treated with PEG-IFN-α-2b. According to whether clinical cure was achieved, the patients were divided into HBsAg clearance group and HBsAg non-clearance group. Related data were collected, including general information and serological/biochemical/virological indicators at different time points during treatment. The independent samples t-test was used for comparison of normally distributed continuous data, and the Mann-Whitney U test was used for comparison of non-normally distributed continuous data; the chi-square test was used for comparison of categorical data. The multivariate logistic regression analysis was used to identify independent influencing factors. The receiver operating characteristic (ROC) curve was used to assess the value of indicators used alone or in combination in predicting clinical cure, and calibration curves were plotted to assess the risk prediction model. Results The univariate analysis showed that there were significant differences between the two groups in age (t=-6.839, P<0.05), history of nucleos(t)ide analogue treatment for over 1 year (χ2=59.339, P<0.05), genotype (χ2=4.610, P<0.05), nonalcoholic fatty liver disease (χ2=5.319, P<0.05), hepatitis B virus DNA status before treatment (χ2=60.861, P <0.05), compensated liver cirrhosis (χ2=10.960, P<0.05), HBeAg status before treatment (χ2=19.060, P<0.05), a history of interferon treatment (χ2=8.162, P<0.05), presence of interferon antibodies after treatment (χ2=12.858, P<0.05), HBsAg level before treatment (Z=-7.412, P<0.05), alanine aminotransaminase (ALT) level at baseline (Z=-6.117, P<0.05), ALT level at 12 weeks of treatment (Z=-7.171, P<0.05), platelet count (PLT) at 24 weeks of treatment (Z=-3.622, P<0.05), and thyroid stimulating hormone (TSH) level at 24 weeks of treatment (Z=-2.830, P<0.05). The multivariate logistic regression analysis showed that age (odds ratio [OR]=1.230, P=0.007), history of nucleos(t)ide analogue treatment for over 1 year (OR=0.008, P=0.011), HBeAg status before treatment (OR=0.003, P=0.012), HBsAg level before treatment (OR=1.005, P=0.014), ALT level at baseline (OR=0.949, P=0.014), ALT level at 12 weeks of treatment (OR=0.969, P=0.016), PLT at 24 weeks of treatment (OR=0.969, P=0.022), and TSH level at 24 weeks of treatment (OR=3.608, P=0.045) were independent influencing factors for HBsAg clearance at 48 weeks of treatment in CHB patients with HBsAg <1 500 IU/mL. The Hosmer-Lemeshow goodness-of-fit test yielded χ2=1.398, P=0.994, indicating that the model had good fitting. The Bootstrap method was used to perform internal validation of the nomogram model, and there was a good degree of fitting between the calibration curve and the ideal curve, with a mean absolute error of 0.029. The ROC curve analysis showed that the combination of predictive factors had an area under the ROC curve of 0.982 (95% confidence interval: 0.961 — 0.999), with a sensitivity of 94.10% and a specificity of 93.10%, suggesting that the nomogram model had a good discriminatory ability. For the CHB patients with HBsAg <1 500 IU/mL and different features, further analysis of HBsAg clearance rate at 48 weeks of treatment showed an HBsAg clearance rate of 69.60% for those with HBsAg ≤67.65 IU/mL before treatment, 58.30% for those with a baseline ALT level of ≥62.50 U/L, 68.30% for those with an ALT level of ≥92.50 U/L at 12 weeks of treatment, 42.40% for those with PLT ≥104×109/L at 24 weeks of treatment, and 48.30% for those with a TSH level of ≤1.38 μIU/mL at 24 weeks of treatment, with significant differences between the two groups (all P<0.001). Conclusion Age, history of nucleos(t)ide analogue treatment for over 1 year, HBeAg status before treatment, HBsAg level before treatment, baseline ALT level, ALT level at 12 weeks of treatment, PLT level at 24 weeks, and TSH level at 24 weeks of treatment are independent predictive factors. The combined prediction nomogram model constructed in this study has a relatively high value in predicting clinical cure at 48 weeks of PEG-IFN-α-2b treatment in CHB patients with HBsAg<1 500 IU/mL, thereby providing a reference for selecting suitable treatment population and predicting clinical cure. -
Key words:
- Hepatitis B, Chronic /
- Interferon-alpha /
- Hepatitis B Surface Antigens /
- Nomograms
-
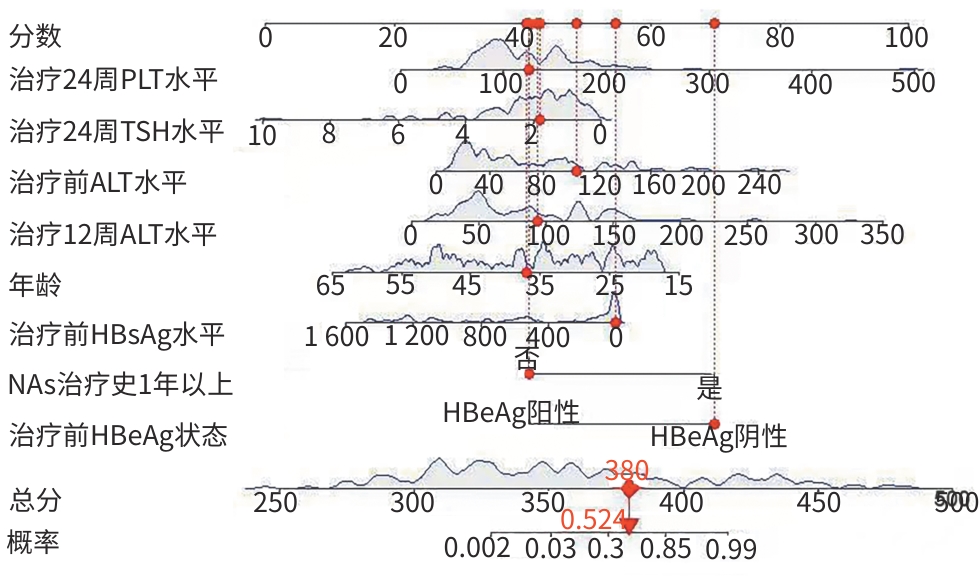
注: CHB,慢性乙型肝炎;NA,核苷(酸)类似物;HBeAg,乙型肝炎e抗原;HBsAg,乙型肝炎表面抗原;PLT,血小板;ALT,丙氨酸氨基转移酶;TSH,促甲状腺激素。
图 1 HBsAg<1 500 IU/mL的CHB患者治疗48周实现HBsAg清除的动态列线图模型
Figure 1. Nomogram model for predicting HBsAg clearance in CHB patients with HBsAg <1 500 IU/mL after 48 weeks of treatment
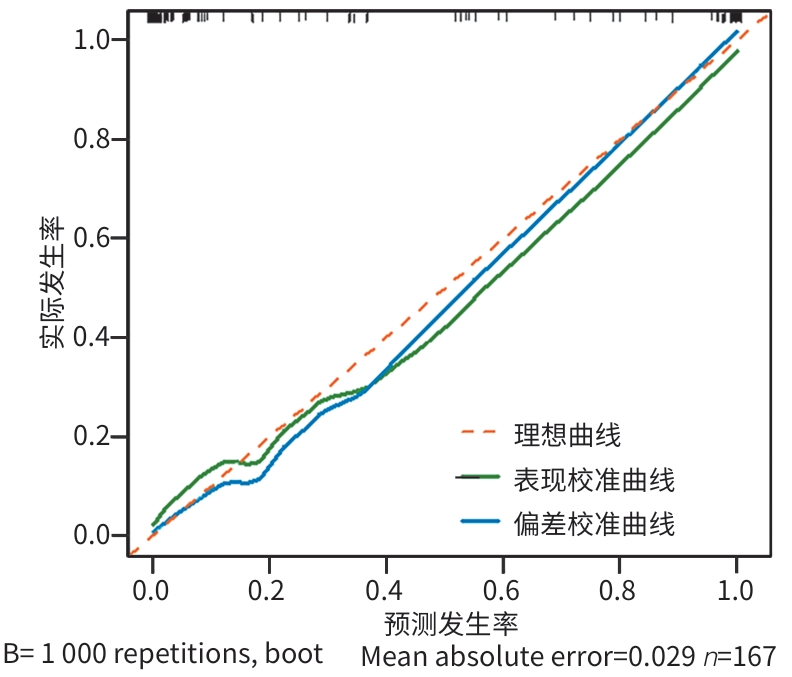
注: CHB,慢性乙型肝炎;HBsAg,乙型肝炎表面抗原。
图 2 列线图模型预测HBsAg<1 500 IU/mL的CHB患者治疗48周实现HBsAg清除的校准曲线
Figure 2. Calibration curve of the Nomogram model for predicting HBsAg clearance in CHB patients with HBsAg<1 500 IU/mL after 48 weeks of treatment
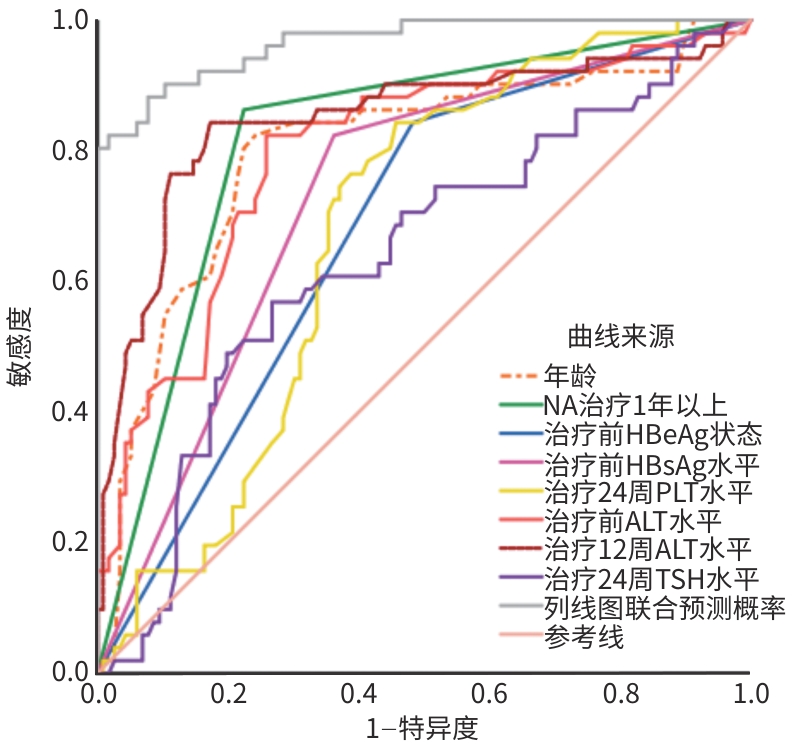
注: CHB,慢性乙型肝炎;NA,核苷(酸)类似物;HBeAg,乙型肝炎e抗原;HBsAg,乙型肝炎表面抗原;PLT,血小板;ALT,丙氨酸氨基转移酶;TSH,促甲状腺激素;ROC曲线,受试者操作特征曲线。
图 3 单个指标以及联合预测模型预测HBsAg<1 500 IU/mL的CHB患者治疗48周实现HBsAg清除的ROC曲线
Figure 3. ROC curves of individual indicators and the combined prediction model for diagnosing HBsAg clearance after 48 weeks of treatment in CHB patients with HBsAg<1 500 IU/mL
表 1 167例HBsAg<1 500 IU/mL的CHB患者基本临床资料比较
Table 1. Comparison of baseline clinical characteristics in 167 CHB patients with HBsAg<1 500 IU/mL
指标 HBsAg清除组(n=51) HBsAg未清除组(n=116) 统计值 P值 性别[例(%)] χ2=0.327 0.567 男 31(60.8) 65(56.0) 女 20(39.2) 51(44.0) 年龄(岁) 28.29±10.01 40.29±10.63 t=-6.839 <0.001 NA治疗史1年以上[例(%)] χ2=59.339 <0.001 是 44(86.3) 26(22.4) 否 7(13.7) 90(77.6) 有IFN治疗史[例(%)] χ2=8.162 0.004 是 22(43.1) 25(21.6) 否 29(56.9) 91(78.4) 基因分型[例(%)] χ2=4.610 0.032 B型 28(54.9) 43(37.1) C型 23(45.1) 73(62.9) 非酒精性脂肪性肝病[例(%)] χ2=5.319 0.021 有 17(33.3) 20(17.2) 无 34(66.7) 96(82.8) 直系三代内肝癌家族史[例(%)] χ2=0.151 0.697 有 11(21.6) 22(19.0) 无 40(78.4) 94(81.0) 代偿期肝硬化[例(%)] χ2=10.960 0.001 有 5(9.8) 40(34.5) 无 46(90.2) 76(65.5) 治疗前HBV DNA状态[例(%)] χ2=60.861 <0.001 阴性 46(90.2) 29(25.0) 阳性 5(9.8) 87(75.0) 治疗前HBeAg状态[例(%)] χ2=19.060 <0.001 阴性 43(84.3) 56(48.3) 阳性 8(15.7) 60(51.7) 治疗前出现IFN抗体[例(%)] χ2=0.658 0.417 是 4(7.8) 14(12.1) 否 47(92.2) 102(87.9) 治疗后出现IFN抗体[例(%)] χ2=12.858 <0.001 是 5(9.8) 43(37.1) 否 46(90.2) 73(62.9) 治疗前HBsAg水平(IU/mL) 91.18(5.47~62.44) 597.35(149.24~1 206.01) Z=-7.412 <0.001 基线水平 WBC(×109/L) 5.32(4.38~6.58) 5.26(4.46~6.25) Z=-0.248 0.804 NEUT(×109/L) 2.88(1.98~4.51) 2.90(2.05~3.75) Z=-0.182 0.855 PLT(×109/L) 226.00(174.00~266.00) 215.50(164.25~260.75) Z=-0.787 0.431 ALT(U/L) 93.00(68.00~145.00) 38.00(23.25~69.50) Z=-6.117 <0.001 TSH(μIU/mL) 2.72(2.16~3.71) 2.89(2.21~4.77) Z=-1.058 0.290 治疗12周水平 WBC(×109/L) 3.12(2.45~4.07) 3.25(3.65~4.16) Z=-1.437 0.151 NEUT(×109/L) 1.32(1.04~1.63) 1.34(0.99~1.85) Z=-0.224 0.823 PLT(×109/L) 125.00(100.00~175.00) 145.00(105.75~195.25) Z=-1.712 0.087 ALT(U/L) 141.00(120.00~156.00) 54.00(42.70~85.00) Z=-7.171 <0.001 TSH(μIU/mL) 2.65(1.46~4.15) 2.54(1.61~4.16) Z=-0.127 0.899  下载: 导出CSV
下载: 导出CSV
Table 1. (continued)
指标 HBsAg清除组(n=51) HBsAg未清除组(n=116) 统计值 P值 治疗24周水平 WBC(×109/L) 2.65(2.47~3.55) 3.15(3.59~3.98) Z=-1.189 0.235 NEUT(×109/L) 0.99(0.84~1.14) 1.04(0.88~1.46) Z=-1.747 0.081 PLT(×109/L) 135.00(115.00~156.00) 100.00(85.00~152.00) Z=-3.622 <0.001 ALT(U/L) 89.00(74.00~103.00) 85.00(60.00~125.00) Z=-0.108 0.914 TSH(μIU/mL) 1.25(0.84~2.43) 1.97(1.28~2.97) Z=-2.830 0.005 注:CHB,慢性乙型肝炎;NA,核苷(酸)类似物;HBV,乙型肝炎病毒;HBeAg,乙型肝炎e抗原;IFN,干扰素;HBsAg,乙型肝炎表面抗原;WBC,白细胞;NEUT,中性粒细胞;PLT,血小板;ALT,丙氨酸氨基转移酶;TSH,促甲状腺激素。
下载: 导出CSV
表 2 HBsAg<1 500 IU/mL的CHB患者治疗48周实现HBsAg清除的多因素Logistic回归分析
Table 2. Multivariate Logistic regression analysis of HBsAg clearance in CHB patients with HBsAg<1 500 IU/mL after 48 weeks of treatment
指标 β SE Wald OR 95%CI P值 年龄 0.207 0.077 7.264 1.230 1.058~1.430 0.007 NA治疗史1年以上 -4.858 1.917 6.423 0.008 0.001~0.332 0.011 有IFN治疗史 -0.878 1.075 0.667 0.415 0.051~3.418 0.414 基因分型 -1.703 1.409 1.460 0.182 0.012~2.883 0.227 非酒精性脂肪性肝病 0.674 1.114 0.366 1.963 0.221~17.436 0.545 代偿期肝硬化 1.680 1.533 1.202 5.367 0.226~108.206 0.273 治疗前HBV DNA状态 -1.978 1.265 2.444 0.138 0.012~1.651 0.118 治疗前HBeAg状态 -5.802 2.299 6.372 0.003 0.001~0.273 0.012 治疗后出现IFN抗体 -2.359 1.647 6.008 0.095 0.004~2.384 0.152 治疗前HBsAg水平 0.005 0.002 6.008 1.005 1.001~1.010 0.014 治疗24周PLT水平 -0.031 0.014 5.258 0.969 0.944~0.995 0.022 基线ALT水平 -0.052 0.021 6.058 0.949 0.910~0.989 0.014 治疗12周ALT水平 -0.031 0.013 5.785 0.969 0.945~0.994 0.016 治疗24周TSH水平 1.283 0.641 4.006 3.608 1.027~12.673 0.045 注:CHB,慢性乙型肝炎;NA,核苷(酸)类似物;HBV,乙型肝炎病毒;HBeAg,乙型肝炎e抗原;IFN,干扰素;HBsAg,乙型肝炎表面抗原;PLT,血小板;ALT,丙氨酸氨基转移酶;TSH,促甲状腺激素;OR,比值比;CI,置信区间。
下载: 导出CSV
表 3 单个指标以及联合预测模型的诊断价值比较
Table 3. Comparison of diagnostic value between individual indicators and combined predictive model
指标 AUC 截断值 约登指数 敏感度(%) 特异度(%) 95%CI Z值 P值 年龄 0.801 34岁 0.583 82.40 75.90 0.722~0.880 -4.631 <0.001 NA治疗史1年以上 0.819 0.639 86.30 77.60 0.758~0.880 -5.745 <0.001 治疗前HBeAg状态 0.680 0.360 84.30 51.70 0.612~0.748 -8.648 <0.001 治疗前HBsAg水平 0.861 67.65 IU/mL 0.627 76.50 86.20 0.795~0.927 -3.771 0.001 基线ALT水平 0.797 62.50 U/L 0.565 82.40 74.10 0.721~0.874 -4.972 <0.001 治疗12周ALT水平 0.849 92.50 U/L 0.671 84.30 82.80 0.774~0.923 -3.918 <0.001 治疗24周PLT水平 0.676 103.50×109/L 0.386 84.30 54.30 0.594~0.758 -7.168 <0.001 治疗24周TSH水平 0.638 1.38 μIU/mL 0.302 56.90 73.30 0.545~0.731 -7.131 <0.001 联合预测因子 0.982 0.872 94.10 93.10 0.961~0.999 注:NA,核苷(酸)类似物;HBeAg,乙型肝炎e抗原;HBsAg,乙型肝炎表面抗原;PLT,血小板;ALT,丙氨酸氨基转移酶;TSH,促甲状腺激素;AUC,受试者操作特征曲线下面积;CI,置信区间。
下载: 导出CSV
表 4 不同特征下CHB患者治疗48周后HBsAg清除率的比较
Table 4. Comparison of HBsAg clearance rates in CHB patients after 48 weeks of treatment under different characteristics
指标 例数 HBsAg清除组 HBsAg未清除组 χ2值 P值 治疗前HBsAg水平[例(%)] 60.733 <0.001 ≤67.65 IU/mL 56 39(69.60) 17(30.40) >67.65 IU/mL 111 12(10.80) 99(89.20) 基线ALT水平[例(%)] 46.094 <0.001 ≥62.50 U/L 72 42(58.30) 30(41.70) <62.50 U/L 95 9(9.50) 86(90.50) 治疗12周ALT水平[例(%)] 67.836 <0.001 ≥92.50 U/L 63 43(68.30) 20(31.70) <92.50 U/L 104 8(7.70) 96(92.30) 治疗24周PLT水平[例(%)] 13.566 <0.001 ≥104×109/L 92 39(42.40) 53(57.60) <104×109/L 75 12(16.00) 63(84.00) 治疗24周TSH水平[例(%)] 13.978 <0.001 ≤1.38 μIU/mL 60 29(48.30) 31(51.70) >1.38 μIU/mL 107 22(20.60) 85(79.40) 注:CHB,慢性乙型肝炎;HBsAg,乙型肝炎表面抗原;ALT,丙氨酸氨基转移酶;PLT,血小板;TSH,促甲状腺激素。
下载: 导出CSV
-
[1] YANG XA, ZHANG K, XU QH, et al. Interferon add-on therapy increased clinical cure significantly for interferon-experienced chronic hepatitis B patients with low HBsAg[J]. Front Immunol, 2022, 13: 997608. DOI: 10.3389/fimmu.2022.997608. [2] LI YP, LIU CR, HE L, et al. Hepatitis B cure: Current situation and prospects[J]. World J Hepatol, 2024, 16( 6): 900- 911. DOI: 10.4254/wjh.v16.i6.900. [3] MO ZS, XIE DY, LIN BL, et al. Therapeutic strategies, practice, and prospect of a clinical cure for chronic hepatitis B in China[J]. Chin J Hepatol, 2024, 32( 5): 411- 417. DOI: 10.3760/cma.j.cn501113-20240325-00156-1.莫志硕, 谢冬英, 林炳亮, 等. 慢性乙型肝炎临床治愈的中国实践、治疗策略和展望[J]. 中华肝脏病杂志, 2024, 32( 5): 411- 417. DOI: 10.3760/cma.j.cn501113-20240325-00156-1. [4] Chinese Society of Hepatology, Chinese Medical Association; Chinese Society of Infectious Diseases, Chinese Medical Association. Guidelines for the prevention and treatment of chronic hepatitis B(version 2022)[J]. J Prac Hepatol, 2023, 26( 3): Posterior Insertion 1-Posterior Insertion 22. DOI: 10.3969/j.issn.1672-5069.2023.03.040.中华医学会肝病学分会, 中华医学会感染病学分会. 慢性乙型肝炎防治指南(2022年版)[J]. 实用肝脏病杂志, 2023, 26( 3): 后插1-后插 22. DOI: 10.3969/j.issn.1672-5069.2023.03.040. [5] ZHANG WH, ZHANG DZ, DOU XG, et al. Consensus on pegylated interferon alpha in treatment of chronic hepatitis B[J]. Chin J Hepatol, 2017, 25( 9): 678- 686. DOI: 10.3760/cma.j.issn.1007-3418.2017.09.007.张文宏, 张大志, 窦晓光, 等. 聚乙二醇干扰素α治疗慢性乙型肝炎专家共识[J]. 中华肝脏病杂志, 2017, 25( 9): 678- 686. DOI: 10.3760/cma.j.issn.1007-3418.2017.09.007. [6] FARAG MS, van CAMPENHOUT MJH, SONNEVELD MJ, et al. Addition of PEG-interferon to long-term nucleos(t)ide analogue therapy enhances HBsAg decline and clearance in HBeAg-negative chronic hepatitis B: Multicentre randomized trial(PAS Study)[J]. J Viral Hepat, 2024, 31( 4): 197- 207. DOI: 10.1111/jvh.13918. [7] WU FP, YANG Y, LI M, et al. Add-on pegylated interferon augments hepatitis B surface antigen clearance vs continuous nucleos(t)ide analog monotherapy in Chinese patients with chronic hepatitis B and hepatitis B surface antigen≤1500 IU/mL: An observational study[J]. World J Gastroenterol, 2020, 26( 13): 1525- 1539. DOI: 10.3748/wjg.v26.i13.1525. [8] JENG WJ, LOK ASF. What will it take to cure hepatitis B?[J]. Hepatol Commun, 2023, 7( 4): e0084. DOI: 10.1097/hc9.0000000000000084. [9] DUSHEIKO G. Hepatitis B cure: How and when[J]. Liver Int, 2021, 41( Suppl 1): 24- 29. DOI: 10.1111/liv.14837. [10] HONG S, HWANG JH, KIM K, et al. Predictive value of HBeAg titer dynamics for HBsAg clearance in pediatric chronic hepatitis B[J]. Front Pediatr, 2025, 13: 1539300. DOI: 10.3389/fped.2025.1539300. [11] WU XL, YAO ZZ, LAI X, et al. Age at treatment initiation predicts response in children with chronic hepatitis B[J]. Aliment Pharmacol Ther, 2023, 58( 9): 866- 873. DOI: 10.1111/apt.17667. [12] YE YM, LIN Y, SUN F, et al. A predictive model for functional cure in chronic HBV patients treated with pegylated interferon alpha: A comparative study of multiple algorithms based on clinical data[J]. Virol J, 2024, 21( 1): 333. DOI: 10.1186/s12985-024-02599-1. [13] SONG KM, ZENG DW, ZHENG YJ, et al. A simple-to-use score system for predicting HBsAg clearance to peginterferon Alfa-2b in nucleoside analogs-experienced chronic hepatitis B patients[J]. Front Med, 2023, 10: 1243202. DOI: 10.3389/fmed.2023.1243202. [14] JIA R, WANG WX, ZHOU ZP, et al. Analysis of the therapeutic efficacy and factors influencing sequential combination of nucleos(t)ide analogues with pegylated interferon alpha for 48~96 weeks in the treatment of patients with chronic hepatitis B[J]. Chin J Hepatol, 2023, 31( 12): 1290- 1296. DOI: 10.3760/cma.j.cn501113-20231124-00227.贾瑞, 王文鑫, 周志平, 等. 核苷(酸)类似物经治慢性乙型肝炎患者序贯联合聚乙二醇干扰素α治疗48~96周的疗效及影响因素分析[J]. 中华肝脏病杂志, 2023, 31( 12): 1290- 1296. DOI: 10.3760/cma.j.cn501113-20231124-00227. [15] JIA R, WANG WX, GAO YY, et al. Early reduction of serum RANTES can predict HBsAg clearance in patients with chronic hepatitis B treated with nucleos(t)ide analogues combined with peginterferon alpha[J]. Chin J Hepatol, 2021, 29( 7): 666- 672. DOI: 10.3760/cma.j.cn501113-20210706-00322.贾瑞, 王文鑫, 高莹莹, 等. 血清RANTES早期下降可预测联合聚乙二醇干扰素α治疗核苷(酸)类似物经治慢性乙型肝炎患者的HBsAg清除[J]. 中华肝脏病杂志, 2021, 29( 7): 666- 672. DOI: 10.3760/cma.j.cn501113-20210706-00322. [16] LIANG H, WANG C, ZHU PF, et al. A study of the clinical curative effect of nucleos(t)ide analogues treated to pegylated interferon-α add-on therapy in patients with chronic hepatitis B[J]. Chin J Hepatol, 2023, 31( 12): 1297- 1305. DOI: 10.3760/cma.j.cn501113-20230505-00206.梁晗, 王晨, 朱鹏飞, 等. 核苷(酸)类似物经治慢性乙型肝炎患者加用聚乙二醇干扰素α治疗的临床治愈效果研究[J]. 中华肝脏病杂志, 2023, 31( 12): 1297- 1305. DOI: 10.3760/cma.j.cn501113-20230505-00206. [17] HU CG, SONG YD, TANG CR, et al. Effect of pegylated interferon plus tenofovir combination on higher hepatitis B surface antigen loss in treatment-naive patients with hepatitis B e antigen-positive chronic hepatitis B: A real-world experience[J]. Clin Ther, 2021, 43( 3): 572- 581. e 3. DOI: 10.1016/j.clinthera.2020.12.022. [18] BRAKENHOFF SM, de MAN RA, BOONSTRA A, et al. Hepatitis B virus RNA decline without concomitant viral antigen decrease is associated with a low probability of sustained response and hepatitis B surface antigen loss[J]. Aliment Pharmacol Ther, 2021, 53( 2): 314- 320. DOI: 10.1111/apt.16172. [19] ZHANG PX, TANG QQ, ZHU J, et al. Predictive models for functional cure in patients with CHB receiving PEG-IFN therapy based on HBsAg quantification through meta-analysis[J]. Hepatol Int, 2024, 18( 4): 1110- 1121. DOI: 10.1007/s12072-024-10666-6. [20] CHEN QX, JIANG XM. Research progress on the factors affecting the clearance of hepatitis B virus surface antigen[J]. Chin J Infect Chemother, 2024, 24( 4): 462- 468. DOI: 10.16718/j.1009-7708.2024.04.014.陈巧霞, 蒋雪梅. 乙型肝炎病毒表面抗原清除影响因素的研究进展[J]. 中国感染与化疗杂志, 2024, 24( 4): 462- 468. DOI: 10.16718/j.1009-7708.2024.04.014. [21] HAN LX, WANG ZL, KANG LY, et al. Predicting relapse after achieving a functional cure for chronic hepatitis B(CHB) using baseline HBsAg and end-of-treatment HBsAb levels[J]. Sci Rep, 2025, 15( 1): 13873. DOI: 10.1038/s41598-025-86555-1. [22] WANG J, FAN T, ZHANG ZY, et al. Incidence and determinants of achieving HBsAg<100 IU/mL in HBeAg-negative CHB patients with nucleos(t)ide analogue treatment[J]. Emerg Microbes Infect, 2025, 14( 1): 2552718. DOI: 10.1080/22221751.2025.2552718. [23] LI K, NING HB, JIN HM, et al. Effect of pegylated interferon α-2b on serum HBsAg clearance rate in treatment of patients with chronic hepatitis B[J]. J Clin Hepatol, 2023, 39( 8): 1819- 1824. DOI: 10.3969/j.issn. 1001-5256.2023.08.009.李宽, 宁会彬, 靳慧鸣, 等. 聚乙二醇干扰素α-2b治疗慢性乙型肝炎患者血清HBsAg清除率的效果分析[J]. 临床肝胆病杂志, 2023, 39( 8): 1819- 1824. DOI: 10.3969/j.issn. 1001-5256.2023.08.009. [24] WANG JL, XI DY, YAN XB, et al. Predictors of HBsAg clearance in HBeAg-negative chronic hepatitis B patients treated with pegylated interferon α-2b and the construction of a nomogram model[J]. J Clin Hepatol, 2023, 39( 12): 2809- 2816. DOI: 10.3969/j.issn.1001-5256.2023.12.010.王佳露, 席德扬, 颜学兵, 等. 聚乙二醇干扰素α-2b治疗HBeAg阴性慢性乙型肝炎患者实现HBsAg清除的预测因素及列线图构建[J]. 临床肝胆病杂志, 2023, 39( 12): 2809- 2816. DOI: 10.3969/j.issn.1001-5256.2023.12.010. [25] WANG WX, JIA R, GAO YY, et al. Quantitative anti-HBc combined with quantitative HBsAg can predict HBsAg clearance in sequential combination therapy with PEG-IFN-α in NA-suppressed chronic hepatitis B patients[J]. Front Immunol, 2022, 13: 894410. DOI: 10.3389/fimmu.2022.894410. [26] HUANG L, ZHANG H, KANG XT, et al. Efficacy of pegylated interferon α-2b plus entecavir therapy and predictors of treatment success in children with chronic hepatitis B[J]. Front Immunol, 2023, 14: 1282922. DOI: 10.3389/fimmu.2023.1282922. [27] LIU HM, GONG HM, TAN ZX, et al. Short-term pegylated interferon alpha in chronic HBV patients with ultra-low HBsAg: A retrospective study[J]. Front Cell Infect Microbiol, 2025, 15: 1582997. DOI: 10.3389/fcimb.2025.1582997. [28] LI H, LIANG S, LIU LL, et al. Clinical cure rate of inactive HBsAg carriers with HBsAg<200 IU/mL treated with pegylated interferon[J]. Front Immunol, 2022, 13: 1091786. DOI: 10.3389/fimmu.2022.1091786. [29] HAN C, JIN LL, ZHU MJ, et al. Efficacy and predictors of pegylated-interferon in hepatitis B surface antigen seroclearance in immune active and inactive chronic hepatitis B patients[J]. J Virus Erad, 2025, 11( 4): 100616. DOI: 10.1016/j.jve.2025.100616. [30] ZHOU DQ, JIA JR, ZHAO F, et al. Determinants of functional cure in interferon-treated chronic hepatitis B: A retrospective cohort analysis of HBsAg dynamics and clinical predictors[J]. Front Cell Infect Microbiol, 2025, 15: 1615327. DOI: 10.3389/fcimb.2025.1615327. [31] WANG WX, JIA R, JIN XY, et al. Serum cytokine change profile associated with HBsAg loss during combination therapy with PEG-IFN-α in NAs-suppressed chronic hepatitis B patients[J]. Front Immunol, 2023, 14: 1121778. DOI: 10.3389/fimmu.2023.1121778. [32] İNKAYA AÇ, TÜRK ARıBAŞ E, KANDEMIR B, et al. Role of tumor necrosis factor alpha promoter polymorphisms in interferon related side effects in chronic hepatitis B patients under interferon alpha 2b treatment[J]. Acta Med, 2019, 50( 2): 32- 38. DOI: 10.32552/2019.actamedica.345. [33] MEI SQ, FENG Y, CUI LL, et al. Thrombotic thrombocytopenic Purpura developed after pegylated interferon treatment for hepatitis B infection[J]. BMC Nephrol, 2022, 23( 1): 400. DOI: 10.1186/s12882-022-03034-9. [34] HUANG CF, YEH ML, HUANG CI, et al. Interference of hepatitis B virus dual infection in platelet count recovery in chronic hepatitis C patients with curative antiviral therapy[J]. J Gastroenterol Hepatol, 2018, 33( 5): 1108- 1114. DOI: 10.1111/jgh.14017. [35] ZHANG P, WANG WX, LI J, et al. CD300A+ CD8+ T cells as predictive biomarkers for achieving functional cure in chronic hepatitis B patients undergoing pegylated interferon-alpha therapy[J]. Aliment Pharmacol Ther, 2025, 62( 5): 512- 525. DOI: 10.1111/apt.70214. [36] LU R, ZHANG M, LIU ZH, et al. Recurrence and influencing factors of hepatitis B surface antigen seroclearance induced by peginterferon alpha-based regimens[J]. World J Gastroenterol, 2024, 30( 44): 4725- 4737. DOI: 10.3748/wjg.v30.i44.4725. [37] WANG T, TANG F, LI FH, et al. Discussion on the duration of response following HBsAg clearance in patients with chronic hepatitis B treated with PegIFNα-2b[J]. Front Immunol, 2025, 16: 1518048. DOI: 10.3389/fimmu.2025.1518048. [38] LIU YS, ZHENG YH, LIN X, et al. Analysis of clinical characteristics of thyroid disorders in patients with chronic hepatitis B treated with pegylated-interferon alpha[J]. BMC Endocr Disord, 2023, 23( 1): 115. DOI: 10.1186/s12902-023-01371-w. -

 本文二维码
本文二维码
计量
- 文章访问数: 219
- HTML全文浏览量: 40
- PDF下载量: 86
- 被引次数: 0

