
 PDF下载 ( 950 KB)
PDF下载 ( 950 KB)

慢性肝病与抑郁障碍的关联性及夜间睡眠时长的中介效应分析
DOI: 10.12449/JCH260418
Analysis of the association between chronic liver disease and depressive disorder and the mediating effect of nocturnal sleep duration
-
摘要:
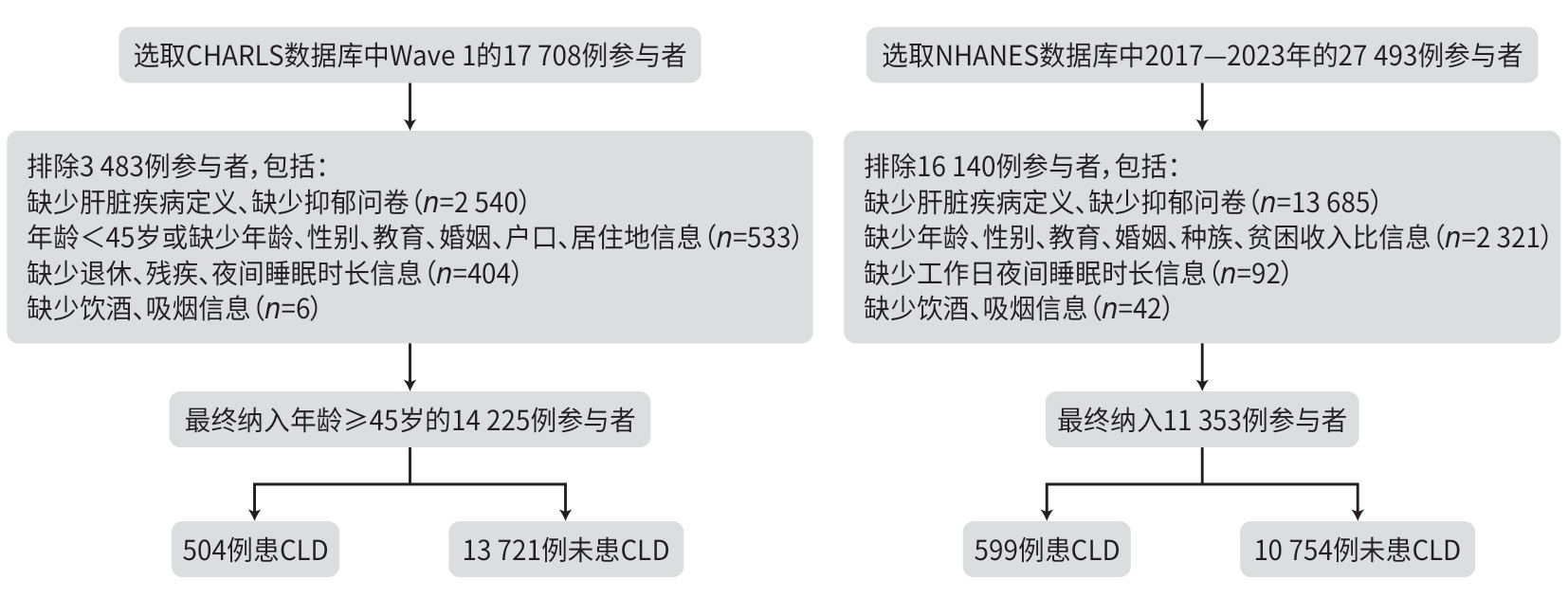
目的 探讨慢性肝病(CLD)与抑郁之间的关联,并分析夜间睡眠时长在其中的中介作用,同时比较该关系在中美人群中的一致性。 方法 整合中国健康与养老追踪调查(CHARLS)(n=14 225)与美国国家健康与营养检查调查(NHANES)(n=11 353)两大数据库,将研究对象分为CLD组与非CLD组,采用递进式Logistic回归模型评估CLD与抑郁的独立关联;以Bootstrap重抽样(1 000次)量化夜间睡眠时长在其中的中介效应比例,并按户籍/种族、收入等分层检验交互效应。计量资料2组间比较采用成组t检验;计数资料组间比较采用χ2检验或Fisher精确检验;采用多因素Logistic回归模型分析不同类型CLD与抑郁的关系。 结果 经多因素校正后,CLD与抑郁风险升高显著关联[CHARLS:比值比(OR)=1.76,95%置信区间(CI):1.46~2.12,P<0.001;NHANES:OR=1.87,95CI:1.50~2.35,P<0.001]。夜间睡眠时长在CLD与抑郁的关联中发挥部分中介作用,在CHARLS和NHANES数据库中的中介效应占比分别为12.41%和2.16%,差异均有统计学意义(P值均<0.05)。交互分析显示,在CHARLS数据库中,CLD与抑郁关联在农业户口人群中更为显著(OR=2.07,95%CI:1.67~2.57,P<0.001);在NHANES中,CLD与抑郁关联在中等贫困收入比人群中更为显著,CLD患者抑郁风险增加(OR=2.66,95% CI:1.92~3.69,P<0.001)。亚型分析表明,自身免疫性肝炎(OR=3.63,95%CI:1.49~8.88,P=0.005)、肝硬化(OR=2.46,95%CI:1.32~4.60,P=0.005)与脂肪肝(OR=1.75,95%CI:1.27~2.39,P=0.001)均显著增加抑郁风险,病毒性肝炎与其他肝病则未达统计学意义(P值均>0.05)。 结论 本研究在人群层面观察到CLD与抑郁之间存在显著关联,并提示夜间睡眠时长在其中可能发挥部分中介作用,该结果在中美人群中具有一致性。研究结果为理解CLD相关抑郁的潜在机制提供了量化参考,并提示在CLD管理中关注睡眠问题具有潜在意义。 Abstract:Objective To investigate the association between chronic liver disease (CLD) and depression and the mediating role of nocturnal sleep duration, as well as the consistency of this association between Chinese and American populations. Methods The data from two databases were integrated, i.e., China Health and Retirement Longitudinal Study (CHARLS) (n=14 225) in China and National Health and Nutrition Examination Survey (NHANES) (n=11 353) in the United States, and the subjects were divided into CLD group and non-CLD group. A stepwise Logistic regression model was used to assess the independent association between CLD and depression. Bootstrap resampling (1 000 times) was used to quantify the proportion of the mediating effect of nocturnal sleep duration, and interaction effects were evaluated through stratified analyses based on the factors including registered residence/race and income. The independent-samples t test was used for comparison of continuous data between two groups; the chi-square test or the Fisher’s exact test was used for comparison of categorical data; a multivariate Logistic regression model analysis was used to investigate the association of different types of CLD with depression. Results After multivariate adjustment, CLD was significantly associated with the increased risk of depression (CHARLS: odds ratio [OR]=1.76, 95% confidence interval [CI]: 1.46 — 2.12, P<0.001; NHANES: OR=1.87, 95%CI: 1.50 — 2.35, P<0.001). Nocturnal sleep duration played a partial mediating role in the association between CLD and depression, with a mediating effect accounted for 12.41% in CHARLS and 2.16% in NHANES (P<0.05). The interaction analysis showed that in CHARLS, the association between CLD and depression was more significant in the residents with agricultural registered permanent residence (OR=2.07, 95%CI: 1.67 — 2.57, P<0.001), and in NHANES, this association was more significant in the population with moderate poverty income ratio (OR=2.66, 95% CI: 1.92 — 3.69, P<0.001). The subtype analysis showed that autoimmune hepatitis (OR=3.63, 95%CI: 1.49 — 8.88, P=0.005), liver cirrhosis (OR=2.46, 95%CI: 1.32 — 4.60, P=0.005), and fatty liver disease (OR=1.75, 95%CI: 1.27 — 2.39, P=0.001) significantly increased the risk of depression, while no statistical significance was observed for viral hepatitis or other liver diseases (P>0.05). Conclusion This study reveals the significant association between CLD and depression at the population level and suggests that nocturnal sleep duration may play a partial mediating role, which is consistent between the Chinese and American populations. These research findings provide quantitative evidence-based support for understanding the underlying mechanism of CLD-related depression and points out the potential significance of sleep issues in CLD management. -
Key words:
- Chronic Liver Disease /
- Sleep /
- Depression /
- Mediation Analysis
-
注: CHARLS,中国健康与养老追踪调查;NHANES,美国国家健康与营养检查调查;CLD,慢性肝病。
图 1 研究人群选择流程图
Figure 1. Flow chart for study population selection
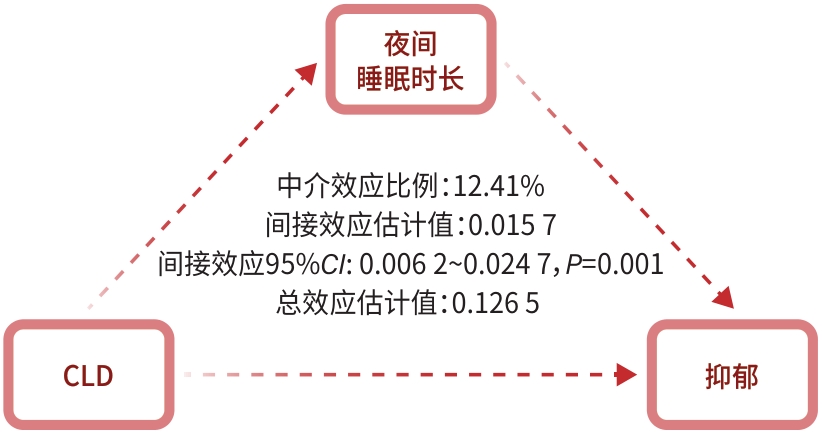
注: CLD,慢性肝病;CHARLS,中国健康与养老追踪调查。
图 2 睡眠时间对CLD与抑郁关联的中介效应分析(CHARLS)
Figure 2. Mediating effect analysis of sleep duration on the association between CLD and depression(CHARLS)
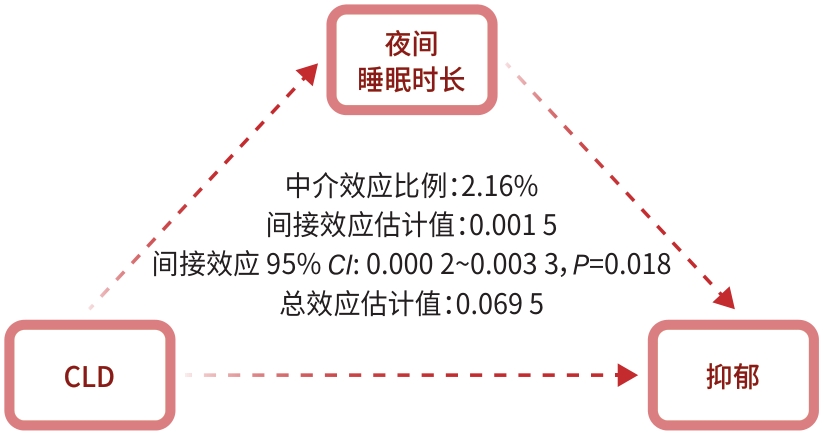
注: CLD,慢性肝病;NHANES,美国国家健康与营养检查调查。
图 3 睡眠时间对CLD与抑郁关联的中介效应分析(NHANES)
Figure 3. Mediating effect analysis of sleep duration on the association between CLD and depression(NHANES)
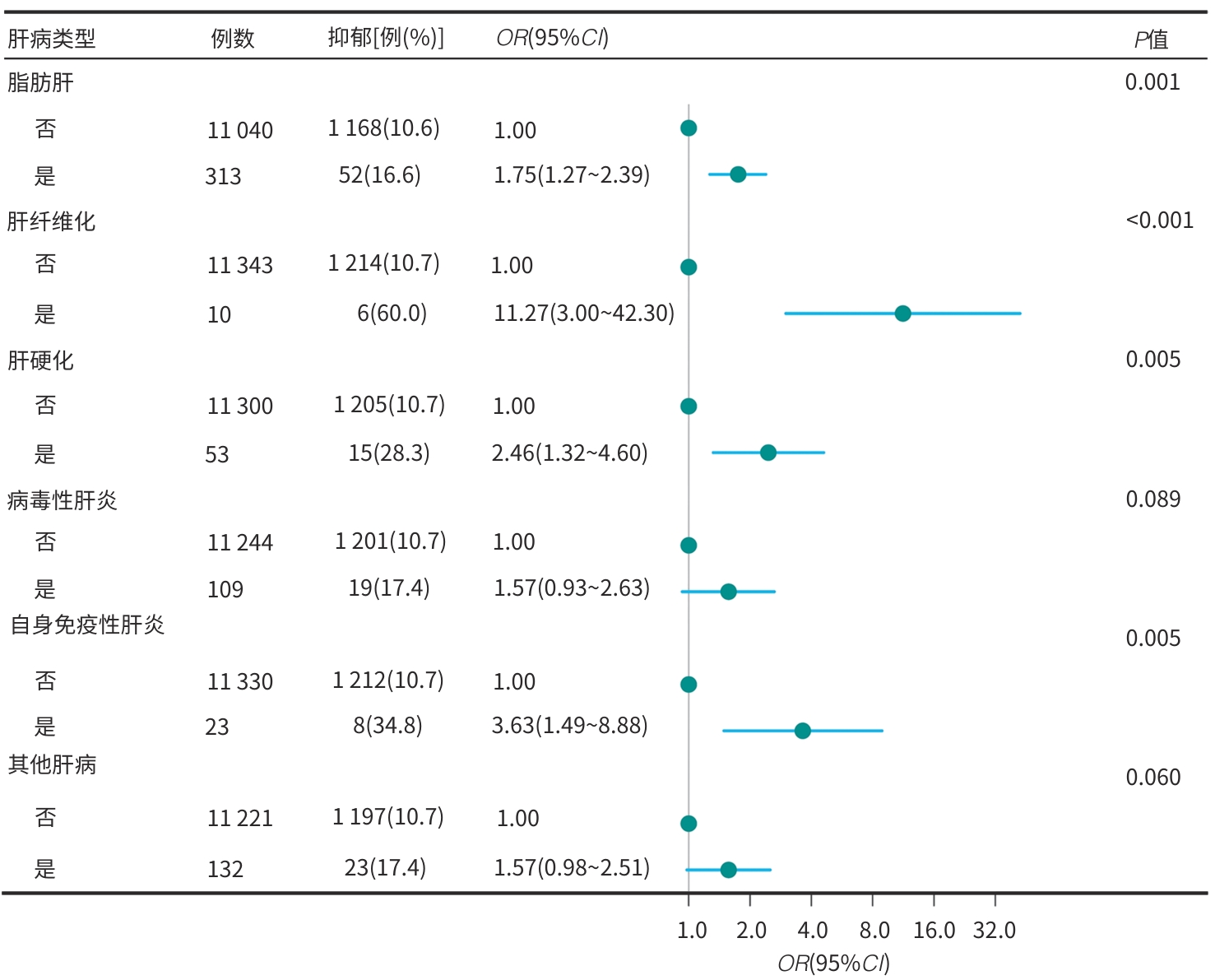
注: CLD,慢性肝病;NHANES,美国国家健康与营养检查调查;OR,比值比;CI,置信区间。
图 4 不同病因CLD与抑郁风险的森林图(NHANES)
Figure 4. Forest plot of depression risk across chronic liver diseases of various etiologies(NHANES)
表 1 CLD和非CLD组基线特征(CHARLS)
Table 1. Baseline characteristics of CLD group and non-CLD group(CHARLS)
变量 总计(n=14 225) 非CLD组(n=13 721) CLD组(n=504) 统计值 P值 年龄(岁) 59.2±9.5 59.2±9.5 59.3±9.1 t=0.067 0.795 性别[例(%)] χ2=7.788 0.005 女 7 275(51.1) 7 048(51.4) 227(45.0) 男 6 950(48.9) 6 673(48.6) 277(55.0) 教育程度[例(%)] χ2=9.314 0.002 文盲 3 713(26.1) 3 611(26.3) 102(20.2) 非文盲 10 512(73.9) 10 110(73.7) 402(79.8) 婚姻[例(%)] 0.749 已婚 11 858(83.4) 11 428(83.3) 430(85.3) 离婚/分居 811(5.7) 786(5.7) 25(5.0) 丧偶 1 440(10.1) 1 394(10.2) 46(9.1) 未婚 116(0.8) 113(0.8) 3(0.6) 户口[例(%)] χ2=4.564 0.033 非农业户口 3 252(22.9) 3 117(22.7) 135(26.8) 农业户口 10 973(77.1) 10 604(77.3) 369(73.2) 居住地[例(%)] χ2=0.846 0.358 城市 5 731(40.3) 5 518(40.2) 213(42.3) 农村 8 494(59.7) 8 203(59.8) 291(57.7) 居住模式[例(%)] χ2=5.389 0.145 农业户口居住农村 8 177(57.5) 7 902(57.6) 275(54.6) 农业户口居住城市 2 796(19.7) 2 702(19.7) 94(18.6) 城市户口居住农村 317(2.2) 301(2.2) 16(3.2) 城市户口居住城市 2 935(20.6) 2 816(20.5) 119(23.6) 退休[例(%)] χ2=20.351 <0.001 否 12 282(86.3) 1 1881(86.6) 401(79.6) 是 1 943(13.7) 1 840(13.4) 103(20.4) 残疾[例(%)] χ2=6.822 0.009 否 11 866(83.4) 11 467(83.6) 399(79.2) 是 2 359(16.6) 2 254(16.4) 105(20.8) 夜间睡眠时长(h) 6.4±1.9 6.4±1.9 6.1±2.0 t=9.647 0.002 饮酒[例(%)] χ2=22.541 <0.001 从未饮酒 8 588(60.4) 8 311(60.6) 277(55.0) 既往饮酒 1 218(8.6) 1 146(8.3) 72(14.3) 目前饮酒 4 419(31.0) 4 264(31.1) 155(30.7) 吸烟[例(%)] χ2=14.241 <0.001 从未吸烟 8 514(59.9) 8 248(60.1) 266(52.8) 既往吸烟 1 302(9.1) 1 237(9.0) 65(12.9) 目前吸烟 4 409(31.0) 4 236(30.9) 173(34.3) 抑郁评分(分) 7.0(3.0~12.0) 7.0(3.0~12.0) 9.0(4.0~15.0) t=39.896 <0.001 抑郁[例(%)] χ2=28.899 <0.001 否 9 007(63.3) 8 745(63.7) 262(52.0) 是 5 218(36.7) 4 976(36.3) 242(48.0) 注:CLD,慢性肝病;CHARLS,中国健康与养老追踪调查。
 下载: 导出CSV
下载: 导出CSV
表 2 CLD和非CLD组基线特征(NHANES)
Table 2. Baseline characteristics of CLD group and non-CLD group(NHANES)
变量 总计(n=11 353) 非CLD组(n=10 754) CLD组(n=599) 统计值 P值 年龄(岁) 52.0±17.3 51.7±17.4 57.2±13.5 t=58.642 <0.001 性别[例(%)] χ2=0.126 0.723 男 5 368(47.3) 5 089(47.3) 279(46.6) 女 5 985(52.7) 5 665(52.7) 320(53.4) 种族[例(%)] χ2=39.168 <0.001 非西班牙裔白人 5 394(47.5) 5 110(47.5) 284(47.4) 非西班牙裔黑人 2 254(19.8) 2 187(20.3) 67(11.2) 墨西哥裔美国人 1 039(9.2) 973(9.1) 66(11.0) 其他 2 666(23.5) 2 484(23.1) 182(30.4) 教育程度[例(%)] χ2=6.746 0.034 <9年 554(4.9) 513(4.8) 41(6.8) 9~12年 3 574(31.5) 3 376(31.4) 198(33.1) >12年 7 225(63.6) 6 865(63.8) 360(60.1) 婚姻[例(%)] χ2=7.684 0.021 已婚/同居 6 459(56.9) 6 104(56.8) 355(59.3) 丧偶/离婚/分居 2 679(23.6) 2 526(23.5) 153(25.5) 从未结婚 2 215(19.5) 2 124(19.7) 91(15.2) PIR[例(%)] χ2=10.129 0.006 ≤1.3 2 813(24.8) 2 638(24.6) 175(29.2) 1.3~3.5 4 347(38.3) 4 112(38.2) 235(39.2) >3.5 4 193(36.9) 4 004(37.2) 189(31.6) 工作日夜间睡眠时长(h) 7.6±1.6 7.6±1.6 7.5±1.8 t=4.360 0.037 吸烟[例(%)] χ2=27.992 <0.001 从未吸烟 6 544(57.6) 6 261(58.2) 283(47.2) 既往吸烟 2 902(25.6) 2 711(25.2) 191(31.9) 目前吸烟 1 907(16.8) 1 782(16.6) 125(20.9) 饮酒[例(%)] χ2=48.330 <0.001 从未饮酒 961(8.5) 915(8.5) 46(7.7) 既往饮酒 2 053(18.1) 1 881(17.5) 172(28.7) 目前饮酒 8 339(73.4) 7 958(74.0) 381(63.6) 抑郁评分(分) 2.0(0.0~5.0) 2.0(0.0~5.0) 3.0(1.0~8.0) t=62.245 <0.001 抑郁[例(%)] χ2=38.261 <0.001 否 10 133(89.3) 9 644(89.7) 489(81.6) 是 1 220(10.7) 1 110(10.3) 110(18.4) 注:CLD,慢性肝病;NHANES,美国国家健康与营养检查调查。
下载: 导出CSV
表 3 CLD与抑郁的逻辑回归分析(CHARLS)
Table 3. Logistic regression analysis of CLD and depression(CHARLS)
变量 例数 抑郁[例(%)] 模型1 模型2 模型3 OR(95%CI) P值 OR(95%CI) P值 OR(95%CI) P值 非CLD 13 721 4 976(36.3) 1.00 1.00 1.00 CLD 504 242(48.0) 1.62(1.36~1.94) <0.001 1.81(1.51~2.18) <0.001 1.76(1.46~2.12) <0.001 注:模型1中未调整变量;模型2中调整年龄、性别、教育、婚姻、户口性质、居住地和居住模式;模型3在模型2的基础上调整了退休、残疾、饮酒和吸烟。CLD,慢性肝病;CHARLS,中国健康与养老追踪调查;OR,比值比;CI,置信区间。
下载: 导出CSV
表 4 CLD与抑郁的逻辑回归分析(NHANES)
Table 4. Logistic regression analysis of CLD and depression(NHANES)
变量 例数 抑郁[例(%)] 模型1 模型2 模型3 OR(95%CI) P值 OR(95%CI) P值 OR(95%CI) P值 非CLD 10 754 1 110(10.3) 1.00 1.00 1.00 CLD 599 110(18.4) 1.95(1.57~2.43) <0.001 1.98(1.58~2.47) <0.001 1.87(1.50~2.35) <0.001 注:模型1中未调整变量;模型2中调整年龄、性别、种族和教育;模型3在模型2的基础上调整了婚姻、贫困收入比、饮酒和吸烟。CLD,慢性肝病;NHANES,美国国家健康与营养检查调查;OR,比值比;CI,置信区间。
下载: 导出CSV
表 5 CLD与抑郁的亚组分析和交互作用分析(CHARLS)
Table 5. Subgroup analysis and interaction of CLD and depression(CHARLS)
亚组 变量 OR(95%CI) P值 P交互 亚组 变量 OR(95%CI) P值 P交互 性别 0.402 吸烟 0.155 女性 非CLD 1.00 从未吸烟 非CLD 1.00 CLD 1.91(1.45~2.53) <0.001 CLD 1.94(1.50~2.51) <0.001 男性 非CLD 1.00 既往吸烟 非CLD 1.00 CLD 1.65(1.27~2.13) <0.001 CLD 1.01(0.58~1.79) 0.962 教育程度 0.263 目前吸烟 非CLD 1.00 文盲 非CLD 1.00 CLD 1.85(1.35~2.54) <0.001 CLD 2.18(1.43~3.33) <0.001 户口性质 0.002 非文盲 非CLD 1.00 非农业 非CLD 1.00 CLD 1.67(1.35~2.07) <0.001 CLD 1.04(0.68~1.57) 0.868 婚姻 0.192 农业 非CLD 1.00 已婚 非CLD 1.00 CLD 2.07(1.67~2.57) <0.001 CLD 1.67(1.36~2.05) <0.001 居住地 0.831 离婚/分居 非CLD 1.00 城市 非CLD 1.00 CLD 2.34(0.98~5.61) 0.056 CLD 1.73(1.29~2.32) <0.001 丧偶 非CLD 1.00 农村 非CLD 1.00 CLD 2.16(1.13~4.12) 0.019 CLD 1.79(1.40~2.29) <0.001 未婚 非CLD 1.00 居住模式 0.006 CLD 12 464 056.581) 0.991 农业户口
居住农村
非CLD 1.00 退休 0.012 CLD 1.88(1.47~2.42) <0.001 否 非CLD 1.00 农业户口
居住城市
非CLD 1.00 CLD 1.97(1.60~2.42) <0.001 CLD 2.75(1.79~4.25) <0.001 是 非CLD 1.00 城市户口
居住农村
非CLD 1.00 CLD 1.03(0.64~1.65) 0.916 CLD 0.55(0.14~2.22) 0.405 饮酒 0.126 城市户口
居住城市
非CLD 1.00 从未饮酒 非CLD 1.00 CLD 1.11(0.72~1.73) 0.633 CLD 2.07(1.61~2.66) <0.001 残疾 0.904 既往饮酒 非CLD 1.00 否 非CLD 1.00 CLD 1.78(1.44~2.20) <0.001 CLD 1.38(0.84~2.29) 0.206 是 非CLD 1.00 目前饮酒 非CLD 1.00 CLD 1.44(1.01~2.06) 0.042 CLD 1.68(1.10~2.56) 0.016 注:1)CLD中未婚患者只有3例,导致样本分布存在完全分离现象,OR值异常增大、置信区间无限扩大,故未提供。CLD,慢性肝病;CHARLS,中国健康与养老追踪调查;OR,比值比;CI,置信区间。
下载: 导出CSV
表 6 CLD与抑郁的亚组分析和交互作用分析(NHANES)
Table 6. Subgroup analysis and interaction of CLD and depression(NHANES)
亚组 变量 OR(95%CI) P值 P交互 性别 0.463 男性 非CLD 1.00 CLD 1.70(1.18~2.45) 0.004 女性 非CLD 1.00 CLD 2.00(1.50~2.67) <0.001 种族 0.042 非西班牙裔白人 非CLD 1.00 CLD 2.20(1.61~3.00) <0.001 非西班牙裔黑人 非CLD 1.00 CLD 3.27(1.79~5.95) <0.001 墨西哥裔美国人 非CLD 1.00 CLD 0.80(0.33~1.94) 0.621 其他 非CLD 1.00 CLD 1.28(0.81~2.03) 0.291 教育程度 0.844 <9年 非CLD 1.00 CLD 1.46(0.63~3.41) 0.382 9~12年 非CLD 1.00 CLD 1.92(1.33~2.76) <0.001 >12年 非CLD 1.00 CLD 1.87(1.38~2.55) <0.001 婚姻 0.981 已婚/与伴侣同居 非CLD 1.00 CLD 1.83(1.32~2.55) <0.001 丧偶/离婚/分居 非CLD 1.00 CLD 1.84(1.23~2.74) 0.003 从未结婚 非CLD 1.00 CLD 1.90(1.16~3.12) 0.011 贫困收入比 0.030 ≤1.3 非CLD 1.00 CLD 1.44(0.98~2.10) 0.062 1.3~3.5 非CLD 1.00 CLD 2.66(1.92~3.69) <0.001 >3.5 非CLD 1.00 CLD 1.28(0.72~2.28) 0.401 吸烟 0.493 从未吸烟 非CLD 1.00 CLD 1.58(1.09~2.28) 0.016 既往吸烟 非CLD 1.00 CLD 1.89(1.25~2.85) 0.003 目前吸烟 非CLD 1.00 CLD 2.33(1.54~3.53) <0.001 饮酒 0.493 从未饮酒 非CLD 1.00 CLD 1.26(0.49~3.24) 0.625 既往饮酒 非CLD 1.00 CLD 1.59(1.04~2.43) 0.031 目前饮酒 非CLD 1.00 CLD 2.09(1.58~2.76) <0.001 注:CLD,慢性肝病;NHANES,美国国家健康与营养检查调查;OR,比值比;CI,置信区间。
下载: 导出CSV
-
[1] LU KQ, SUI JJ, YU WH, et al. An analysis of the burden of liver cirrhosis: Differences between the global, China, the United States and India[J]. Liver Int, 2024, 44( 12): 3183- 3203. DOI: 10.1111/liv.16087. [2] DEVARBHAVI H, ASRANI SK, ARAB JP, et al. Global burden of liver disease: 2023 update[J]. J Hepatol, 2023, 79( 2): 516- 537. DOI: 10.1016/j.jhep.2023.03.017. [3] KARLSEN TH, SHERON N, ZELBER-SAGI S, et al. The EASL-Lancet Liver Commission: Protecting the next generation of Europeans against liver disease complications and premature mortality[J]. Lancet, 2022, 399( 10319): 61- 116. DOI: 10.1016/S0140-6736(21)01701-3. [4] KRONSTEN VT, SHAWCROSS DL. Clinical implications of inflammation in patients with cirrhosis[J]. Am J Gastroenterol, 2025, 120( 1): 65- 74. DOI: 10.14309/ajg.0000000000003056. [5] HARTL L, SIMBRUNNER B, JACHS M, et al. Lower free triiodothyronine(fT3) levels in cirrhosis are linked to systemic inflammation, higher risk of acute-on-chronic liver failure, and mortality[J]. JHEP Rep, 2023, 6( 1): 100954. DOI: 10.1016/j.jhepr.2023.100954. [6] JALAN R, D'AMICO G, TREBICKA J, et al. New clinical and pathophysiological perspectives defining the trajectory of cirrhosis[J]. J Hepatol, 2021, 75( Suppl 1): S14- S26. DOI: 10.1016/j.jhep.2021.01.018. [7] LEE SS, YOO YC. NOX-NOS crosstalk in the liver-brain axis: Novel insights for redox regulation and neurodegenerative diseases[J]. Redox Biol, 2025, 86: 103807. DOI: 10.1016/j.redox.2025.103807. [8] KRONSTEN VT, TRANAH TH, PARIANTE C, et al. Gut-derived systemic inflammation as a driver of depression in chronic liver disease[J]. J Hepatol, 2022, 76( 3): 665- 680. DOI: 10.1016/j.jhep.2021.11.008. [9] SHAHEEN AA, KAPLAN GG, SHARKEY KA, et al. Impact of major depression and antidepressant use on alcoholic and non-alcoholic fatty liver disease: A population-based study[J]. Liver Int, 2021, 41( 10): 2308- 2317. DOI: 10.1111/liv.14973. [10] MARJOT T, RAY DW, WILLIAMS FR, et al. Sleep and liver disease: A bidirectional relationship[J]. Lancet Gastroenterol Hepatol, 2021, 6( 10): 850- 863. DOI: 10.1016/S2468-1253(21)00169-2. [11] ZIMBREAN PC, JAKAB SS. Depression and anxiety management in cirrhosis[J]. Hepatol Commun, 2024, 9( 1): e0600. DOI: 10.1097/HC9.0000000000000600. [12] KIM M, LIOTTA EM, MAAS MB, et al. Rest-activity rhythm disturbance in liver cirrhosis and association with cognitive impairment[J]. Sleep, 2021, 44( 6): zsaa288. DOI: 10.1093/sleep/zsaa288. [13] ZHAO YH, HU YS, SMITH JP, et al. Cohort profile: The China health and retirement longitudinal study(CHARLS)[J]. Int J Epidemiol, 2014, 43( 1): 61- 68. DOI: 10.1093/ije/dys203. [14] LARSEN A, PINTYE J, ODHIAMBO B, et al. Comparing depression screening tools(CESD-10, EPDS, PHQ-9, and PHQ-2) for diagnostic performance and epidemiologic associations among postpartum Kenyan women: Implications for research and practice[J]. J Affect Disord, 2023, 324: 637- 644. DOI: 10.1016/j.jad.2022.12.101. [15] TANG L, YIN RY, HU Q, et al. The effect of childhood socioeconomic status on depressive symptoms in middle-old age: The mediating role of life satisfaction[J]. BMC Psychiatry, 2022, 22( 1): 398. DOI: 10.1186/s12888-022-04046-3. [16] KROENKE K, SPITZER RL, WILLIAMS JB. The PHQ-9: Validity of a brief depression severity measure[J]. J Gen Intern Med, 2001, 16( 9): 606- 613. DOI: 10.1046/j.1525-1497.2001.016009606.x. [17] COOPER KM, COLLETTA A, OSORIO B, et al. History of depression is associated with higher prevalence of hepatic encephalopathy in patients with advanced liver disease[J]. Am J Med, 2024, 137( 9): 872- 879. e 2. DOI: 10.1016/j.amjmed.2024.04.036. [18] WUNSCH E, KRAUSE L, GEVERS TJ, et al. Confidence in treatment is contributing to quality of life in autoimmune liver diseases. The results of ERN RARE-LIVER online survey[J]. Liver Int, 2023, 43( 2): 381- 392. DOI: 10.1111/liv.15440. [19] ALRABADI LS, DUTTON A, RABIEE A, et al. Mindfulness-based stress reduction may decrease stress, disease activity, and inflammatory cytokine levels in patients with autoimmune hepatitis[J]. JHEP Rep, 2022, 4( 5): 100450. DOI: 10.1016/j.jhepr.2022.100450. [20] FENG Q, IZZI-ENGBEAYA CN, MANOUSOU P, et al. Obesity drives the link between liver fat and depression: Cross-sectional and prospective investigations[J]. Diabetes Obes Metab, 2025, 27( 9): 5127- 5134. DOI: 10.1111/dom.16562. [21] ÅSTRÖM H, SHANG Y, HAGSTRÖM H, et al. Persons with metabolic dysfunction-associated steatotic liver disease are at increased risk of severe depression[J]. Liver Int, 2024, 44( 10): 2551- 2563. DOI: 10.1111/liv.16019. [22] KARDASHIAN A, SERPER M, TERRAULT N, et al. Health disparities in chronic liver disease[J]. Hepatology, 2023, 77( 4): 1382- 1403. DOI: 10.1002/hep.32743. [23] LEDENKO M, PATEL T. Poverty traps and mortality from liver diseases in the United States[J]. Am J Gastroenterol, 2024, 119( 12): 2462- 2470. DOI: 10.14309/ajg.0000000000002899. -

 本文二维码
本文二维码
计量
- 文章访问数: 202
- HTML全文浏览量: 119
- PDF下载量: 70
- 被引次数: 0

