
 PDF下载 ( 13180 KB)
PDF下载 ( 13180 KB)

布-加综合征病因和诊疗模式的东西方差异
DOI: 10.12449/JCH260403
Differences in the etiology and diagnostic and therapeutic mode of Budd-Chiari syndrome between China and Western countries
-
摘要: 布‑加综合征(BCS)是指肝静脉和/或其开口近端的下腔静脉发生阻塞,继而引发门静脉和/或下腔静脉高压的一组临床综合征。既往研究显示,BCS在不同地区人群中的病因构成、临床分型以及治疗策略存在显著差异。西方国家BCS多继发于骨髓增殖性肿瘤等血栓性疾病,病变以肝静脉阻塞为主;治疗上多遵循“抗凝-开通-分流-肝移植”的阶梯式策略,经颈静脉肝内门体分流术的介入时机相对较早。相比之下,中国BCS更常见于肝后段下腔静脉膜性阻塞及混合型阻塞,经皮腔内血管成形术在治疗体系中占据核心地位。上述差异可能与遗传背景、环境暴露以及医疗实践模式等多重因素相关,并对临床决策路径与预后评估产生重要影响。本文基于文献梳理,系统总结BCS的地域异质性特征,旨在为临床医师提供跨地域的诊疗参考,并为未来围绕BCS地域差异开展国际合作研究提供线索与方向。Abstract: Budd-Chiari syndrome (BCS) is a clinical syndrome of portal vein and/or inferior vena cava (IVC) hypertension caused by obstruction of the hepatic veins and/or the IVC proximal to its opening. Previous studies have shown that there are significant differences in the etiology, clinical classification, and therapeutic strategy of BCS across different regions. In Western countries, BCS is often secondary to thrombotic disorders, especially myeloproliferative neoplasms, with hepatic vein obstruction as the main lesion; the treatment of BCS mainly follows a stepwise strategy of anticoagulation, recanalization, shunting, and liver transplantation, with relatively early timing for transjugular intrahepatic portosystemic shunt. In contrast, BCS in China mainly involves membranous obstruction of the retrohepatic IVC and mixed-type obstruction, and percutaneous transluminal angioplasty is the core treatment method for BCS. These differences may be associated with various factors such as genetic background, environmental exposure, and healthcare practice patterns, with a significant impact on clinical decision-making and prognostic assessment. This article systematically summarizes the geographic heterogeneity of BCS through a literature review, so as to provide a cross-regional diagnostic and therapeutic reference for clinicians, as well as clues and directions for international collaborative research on the regional differences of BCS in the future.
-
Key words:
- Budd-Chiari Syndrome /
- Etiology /
- Therapeutics
-
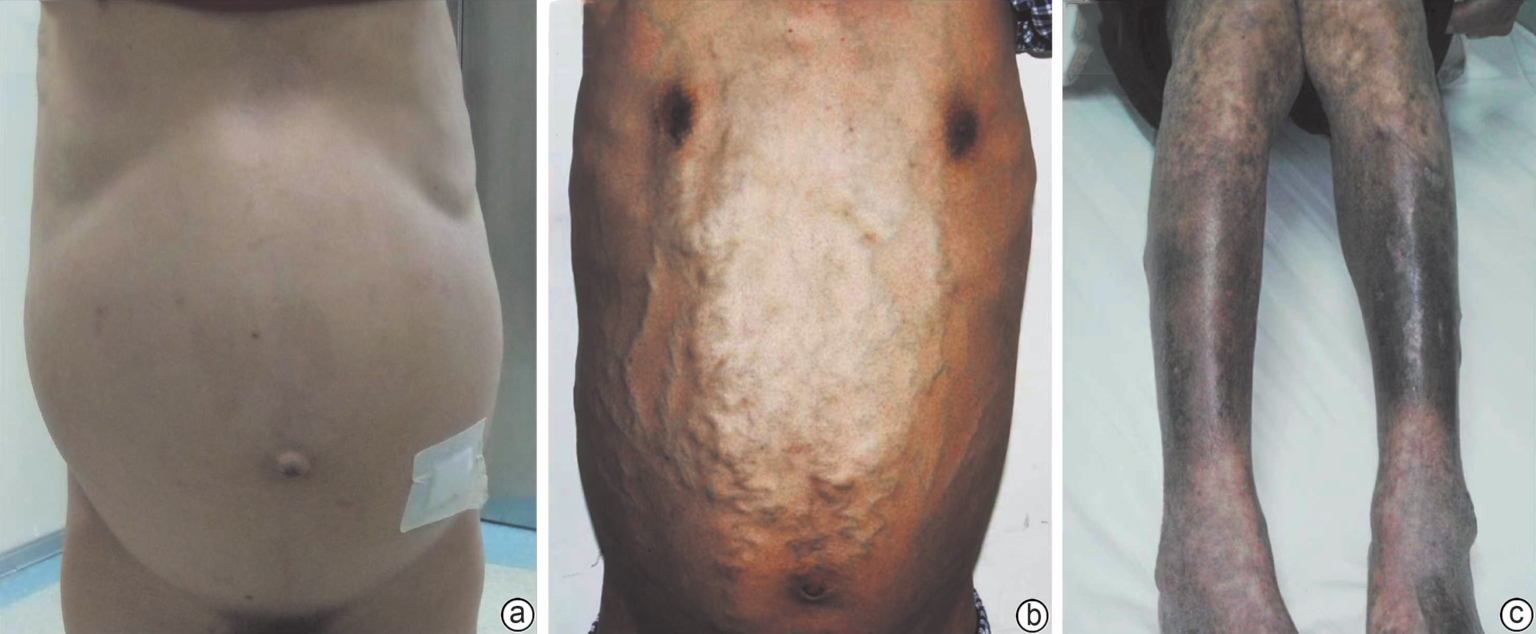
注: a,肝静脉阻塞引起的严重腹水;b,因下腔静脉阻塞导致的腹壁静脉曲张;c,下腔静脉阻塞所致双下肢皮肤色素沉着。
图 1 BCS患者的临床表现
Figure 1. The clinical manifestations of patients with Budd-Chiari syndrome
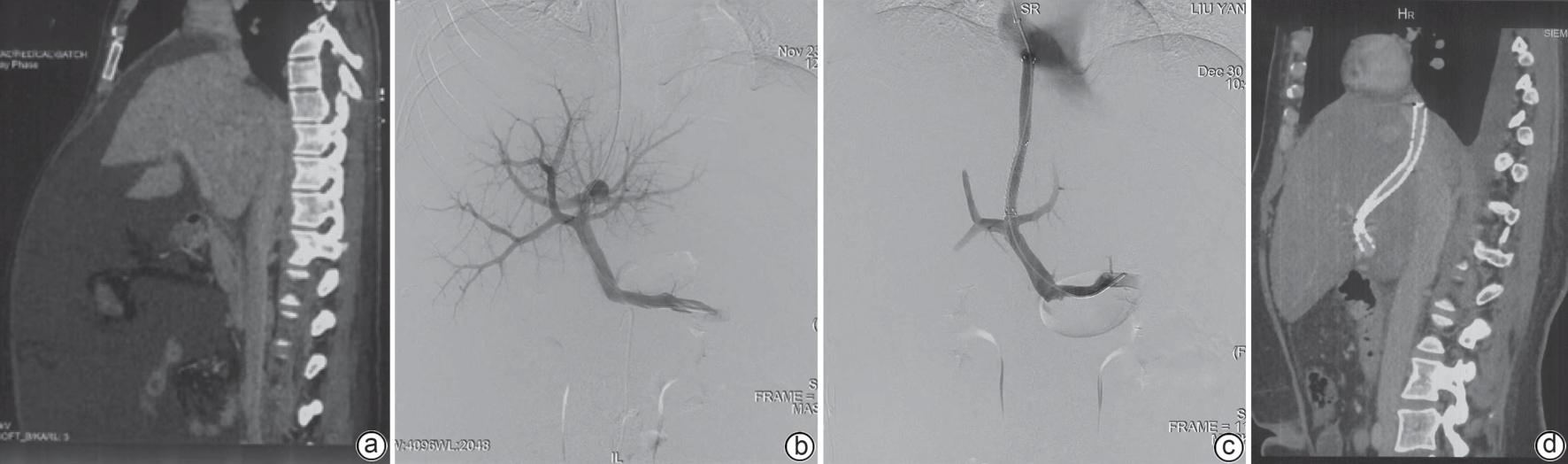
注: a,术前:CT提示肝脏肿大、腹水,同时伴有黄疸;b,术中:从下腔静脉穿刺门静脉左支根部,直接门静脉造影显示门脾静脉通畅,血流缓慢,测门静脉压力梯度为23 mmHg;c,术中:成功建立TIPS分流道后,造影证实血流速度明显加快,门静脉压力梯度降至10 mmHg;d,术后随访:术后1个月CT显示肝脏形态显著改善,腹水完全消失。CT,计算机体层成像;TIPS,经颈静脉肝内门体分流术。
图 2 TIPS治疗肝静脉型BCS的流程与疗效
Figure 2. The procedure and efficacy of TIPS in the treatment of hepatic vein type Budd-Chiari syndrome
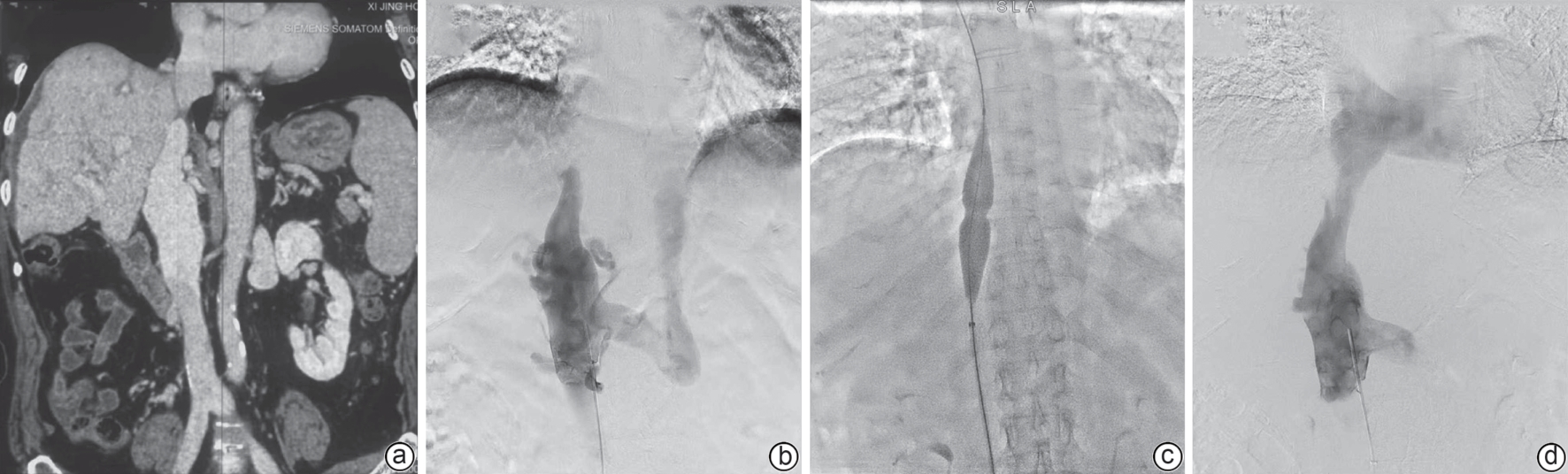
注: a,术前:CT三维重建显示肝脏肿大、淤血,下腔静脉近心端狭窄、远心端扩张;b,术中:静脉造影证实狭窄处为完全闭塞,血流中断,并可见扩张的侧支血管,测压为25 mmHg;c,术中:使用造影导丝硬头端锐性开通下腔静脉闭塞处,交换成硬导丝,使用球囊(直径24 mm)对闭塞段进行扩张;d,术后:复查造影显示下腔静脉血流通畅,侧支血管消失,压力降至9 mmHg。CT,计算机体层成像;PTA,经皮腔内血管成形术。
图 3 下腔静脉型BCS的PTA治疗过程
Figure 3. PTA treatment process in inferior vena cava type Budd-Chiari syndrome
表 1 BCS临床参数的东西方差异
Table 1. Differences of Budd-Chiari syndrome between East and West
项目 东方 西方 病因 膜性阻塞 获得性或遗传性血栓
性疾病分型 以下腔静脉型或混合
型为主以肝静脉型为主 临床表现 双下肢水肿、色素沉
着、溃烂和胸腹壁静脉
曲张肝脏肿大、腹水和黄疸 治疗策略 以血管开通治疗(球囊
扩张/支架植入)为主以TIPS治疗为主 预后 肝癌风险高 急性肝衰竭的风险
较高 下载: 导出CSV
下载: 导出CSV
-
[1] MONTES LÓPEZ AK, GARCIA RUEDA JE, HERRERA CORREA D, et al. Pathophysiology of primary budd-chiari syndrome: A narrative review[J]. Cureus, 2025, 17( 11): e96539. DOI: 10.7759/cureus.96539. [2] LI YY, DE STEFANO V, LI HY, et al. Epidemiology of Budd-Chiari syndrome: A systematic review and meta-analysis[J]. Clin Res Hepatol Gastroenterol, 2019, 43( 4): 468- 474. DOI: 10.1016/j.clinre.2018.10.014. [3] European Association for the Study of the Liver. EASL clinical practice guidelines on vascular diseases of the liver[J]. J Hepatol, 2026, 84( 2): 399- 456. DOI: 10.1016/j.jhep.2025.08.001. [4] QI XS, REN WR, de STEFANO V, et al. Associations of coagulation factor V Leiden and prothrombin G20210A mutations with Budd-Chiari syndrome and portal vein thrombosis: A systematic review and meta-analysis[J]. Clin Gastroenterol Hepatol, 2014, 12( 11): 1801- 1812.e7. DOI: 10.1016/j.cgh.2014.04.026. [5] ZHANG W, QI X, ZHANG XT, et al. Budd-chiari syndrome in China: A systematic analysis of epidemiological features based on the Chinese literature survey[J]. Gastroenterol Res Pract, 2015, 2015: 738548. DOI: 10.1155/2015/738548. [6] QI X, HAN G, GUO X, et al. Review article: The aetiology of primary Budd-Chiari syndrome- differences between the West and China[J]. Aliment Pharmacol Ther, 2016, 44( 11-12): 1152- 1167. DOI: 10.1111/apt.13815. [7] WANG H, SUN GX, ZHANG PJ, et al. JAK2 V617F mutation and 46/1 haplotype in Chinese Budd-Chiari syndrome patients[J]. J Gastroenterol Hepatol, 2014, 29( 1): 208- 214. DOI: 10.1111/jgh.12379. [8] FAN JH, WANG QH, LUO BH, et al. Prevalence of prothrombotic factors in patients with Budd-Chiari syndrome or non-cirrhotic nonmalignant portal vein thrombosis: A hospital-based observational study[J]. J Gastroenterol Hepatol, 2020, 35( 7): 1215- 1222. DOI: 10.1111/jgh.14925. [9] QI X, WU F, REN W, et al. Thrombotic risk factors in Chinese Budd-Chiari syndrome patients. An observational study with a systematic review of the literature[J]. Thromb Haemost, 2013, 109( 5): 878- 884. DOI: 10.1160/TH12-10-0784. [10] Expert Committee on Vane Cava Obstruction, Specialized Committee of Endovascology, Chinese Medical Doctor Association. Expert consensus on the classification of subtype in Budd-Chiari syndrome[J]. J Clin Hepatol, 2017, 33( 7): 1229- 1235. DOI: 10.3969/j.issn.1001-5256.2017.07.005.中国医师协会腔内血管学专业委员会腔静脉阻塞专家委员会. 布-加综合征亚型分型的专家共识[J]. 临床肝胆病杂志, 2017, 33( 7): 1229- 1235. DOI: 10.3969/j.issn.1001-5256.2017.07.005. [11] SHUKLA A, SHRESHTHA A, MUKUND A, et al. Budd-Chiari syndrome: Consensus guidance of the Asian Pacific Association for the study of the liver(APASL)[J]. Hepatol Int, 2021, 15( 3): 531- 567. DOI: 10.1007/s12072-021-10189-4. [12] SEIJO S, PLESSIER A, HOEKSTRA J, et al. Good long-term outcome of Budd-Chiari syndrome with a step-wise management[J]. Hepatology, 2013, 57( 5): 1962- 1968. DOI: 10.1002/hep.26306. [13] WANG QH, LI K, HE CY, et al. Angioplasty with versus without routine stent placement for Budd-Chiari syndrome: A randomised controlled trial[J]. Lancet Gastroenterol Hepatol, 2019, 4( 9): 686- 697. DOI: 10.1016/S2468-1253(19)30177-3. [14] ZHANG W, WANG QZ, CHEN XW, et al. Budd-Chiari syndrome in China: A 30-year retrospective study on survival from a single center[J]. World J Gastroenterol, 2018, 24( 10): 1134- 1143. DOI: 10.3748/wjg.v24.i10.1134. [15] WANG QZ, ZHANG W, CHEN XW, et al. Percutaneous recanalization for Budd-Chiari syndrome: Long-term outcomes in 141 Chinese patients[J]. J China Clin Med Imag, 2019, 30( 8): 586- 590. DOI: 10.12117/jccmi.2019.08.014.王巧争, 张伟, 陈晓伟, 等. 布-加综合征的介入治疗: 141例患者的远期疗效分析[J]. 中国临床医学影像杂志, 2019, 30( 8): 586- 590. DOI: 10.12117/jccmi.2019.08.014. [16] XIA DD, LUO BH, ZHANG CQ, et al. Interventional radiological management for budd-chiari syndrome: A 10-year retrospective, multicenter survey on 997 patients in China[J]. Clin Gastroenterol Hepatol, 2025. DOI: 10.1016/j.cgh.2025.07.004.[ Online ahead of print] [17] ASL AA, LANKARANI KB, NIKEGHBALIAN S, et al. Post liver transplant complications of Budd-Chiari syndrome[J]. Indian J Gastroenterol, 2021, 40( 3): 281- 286. DOI: 10.1007/s12664-020-01139-3. [18] HIDAKA M, EGUCHI S. Budd-Chiari syndrome: Focus on surgical treatment[J]. Hepatol Res, 2017, 47( 2): 142- 148. DOI: 10.1111/hepr.12752. -

 本文二维码
本文二维码
计量
- 文章访问数: 220
- HTML全文浏览量: 86
- PDF下载量: 100
- 被引次数: 0

