
 PDF下载 ( 1875 KB)
PDF下载 ( 1875 KB)

肝移植术后并发急性肾损伤的危险因素及预测模型构建
DOI: 10.12449/JCH260218
Risk factors for acute kidney injury after liver transplantation and establishment of a predictive model
-
摘要:
目的 探讨肝移植术后发生急性肾损伤(AKI)的影响因素,构建并验证其风险预测模型,为临床早期识别高危患者和干预提供依据。 方法 采用单中心、回顾性研究方法,收集2020年3月—2025年6月于山西医科大学第一医院肝脏移植中心行肝移植手术的162例患者的临床资料。根据改善全球肾脏病预后组织共识的AKI诊断标准,按照术后7 d内AKI的发生情况,将患者分为AKI组(n=69)和非AKI组(n=93)。符合正态分布的计量资料组间比较采用成组t检验;非正态分布的计量资料组间比较采用Mann-Whitney U检验;计数资料两组间比较采用χ2检验或Fisher确切概率法。采用单因素差异分析筛选与肝移植术后AKI相关的因素,多因素Logistic回归筛选出独立危险因素,并建立列线图模型,采用Bootstrap法重复抽样1 000次,对模型进行内部验证,将数据集按照7∶3随机分为训练集(n=113)和验证集(n=49),通过受试者操作特征曲线、校准曲线和决策曲线分析评估预测模型的区分度、校准度和临床适用性。 结果 肝移植术后AKI的独立危险因素包括体重指数[比值比(OR)=1.281,95%置信区间(CI):1.037~1.582,P=0.022]、血肌酐(OR=1.097,95%CI:1.020~1.181,P=0.013)、术中出血量(OR=1.005,95%CI:1.002~1.009,P=0.004)和冷缺血时间(OR=0.984,95%CI:0.976~0.991,P<0.001)。根据上述因素构建列线图预测模型,受试者操作特征曲线下面积(AUC)为0.964(95%CI:0.931~0.997),最佳截断值为0.319,灵敏度为0.971,特异度为0.903。在训练集中,列线图的AUC为0.969(95%CI:0.933~0.971);验证集中的AUC为0.941(95%CI:0.855~0.944),校准曲线显示预测发生率和实际发生率具有较好的一致性,决策曲线分析显示模型具有良好的临床净获益。 结论 体重指数、血肌酐、冷缺血时间和术中出血量是肝移植术后发生AKI的独立危险因素,基于此构建的列线图预测模型表现良好,对肝移植术后AKI的发生有较好的预测价值。 Abstract:Objective To investigate the risk factors for acute kidney injury (AKI) after liver transplantation, and to establish and validate a risk prediction model, and to provide a basis for early identification of high-risk patients and intervention in clinical practice. Methods A single-center retrospective study was conducted, and clinical data were collected from 162 patients who received liver transplantation in Liver Transplantation Center of The First Hospital of Shanxi Medical University from March 2020 to June 2025. The patients were divided into AKI group with 69 patients and non-AKI group with 93 patients according to the diagnostic criteria for AKI established by the Kidney Disease: Improving Global Outcomes organization and the presence or absence of AKI within 7 days after surgery. The independent-samples t test was used for comparison of normally distributed continuous data between groups, while the Mann-Whitney U test was used for comparison of non-normally distributed continuous data between groups, and the chi-square test or the Fisher’s exact test was used for comparison of categorical data between groups. The univariate differential analysis was used to obtain the factors associated with AKI after liver transplantation, and the multivariate logistic regression analysis was used to identify the independent risk factors and establish a nomogram model; the Bootstrap method with 1 000 repeated samples was used to perform internal validation of the model. The dataset was randomly divided into a training set and a validation set at a ratio of 7∶3, and the receiver operating characteristic (ROC) curve, the calibration curve, and decision curve analysis (DCA) were used to assess the discriminatory ability, calibration, and clinical applicability of the predictive model. Results Body mass index (BMI) (odds ratio [OR]=1.281, 95% confidence interval [CI]: 1.037 — 1.582, P=0.022), serum creatinine (OR=1.097, 95%CI: 1.020 — 1.181, P=0.013), intraoperative blood loss (OR=1.005, 95%CI: 1.002 — 1.009, P=0.004), and cold ischemia time (OR=0.984, 95%CI: 0.976 — 0.991, P<0.001) were independent risk factors for the development of AKI after liver transplantation. The nomogram prediction model established based on the above factors had an area under the ROC curve (AUC) of 0.964 (95%CI: 0.931 — 0.997), with an optimal cutoff value of 0.319, a sensitivity of 0.971, and a specificity of 0.903. In the training set (n=113), the nomogram had an AUC of 0.969 (95% CI: 0.933 — 0.971), while in the validation set (n=49), the nomogram had an AUC of 0.941 (95%CI: 0.855 — 0.944). The calibration curve showed good consistency between the predicted incidence rate and the actual incidence rate, and DCA showed that it had good net clinical benefit. Conclusion BMI, serum creatinine, cold ischemia time, and intraoperative blood loss are independent risk factors for the development of AKI after liver transplantation, and the nomogram prediction model established based on these factors performs well and has a good value in predicting the development of AKI after liver transplantation. -
Key words:
- Liver Transplantation /
- Acute Kidney Injury /
- Nomograms
-
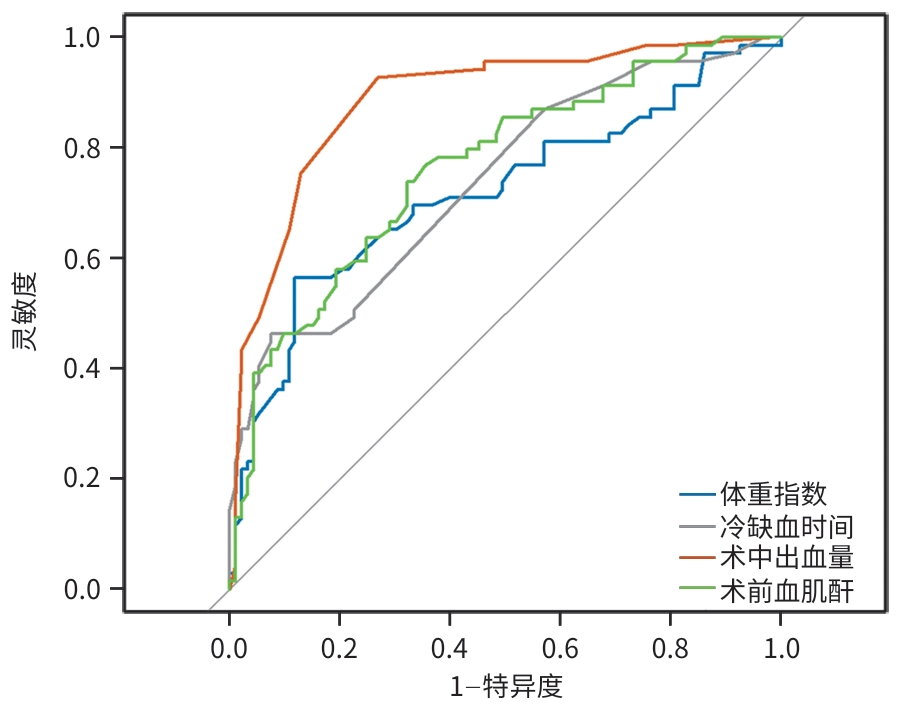
注: AKI,急性肾损伤;ROC曲线,受试者操作特征曲线。
图 1 肝移植术后AKI的ROC曲线
Figure 1. ROC curve for AKI after liver transplantation
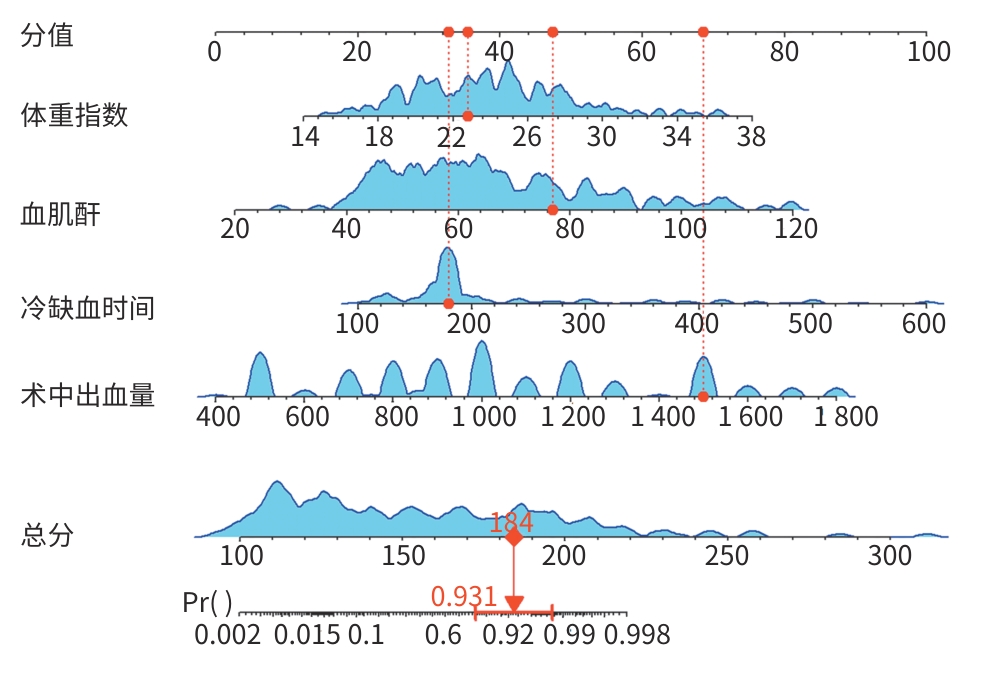
注: AKI,急性肾损伤。
图 2 肝移植术后AKI的列线图预测模型
Figure 2. Nomogram prediction model for AKI after liver transplantation
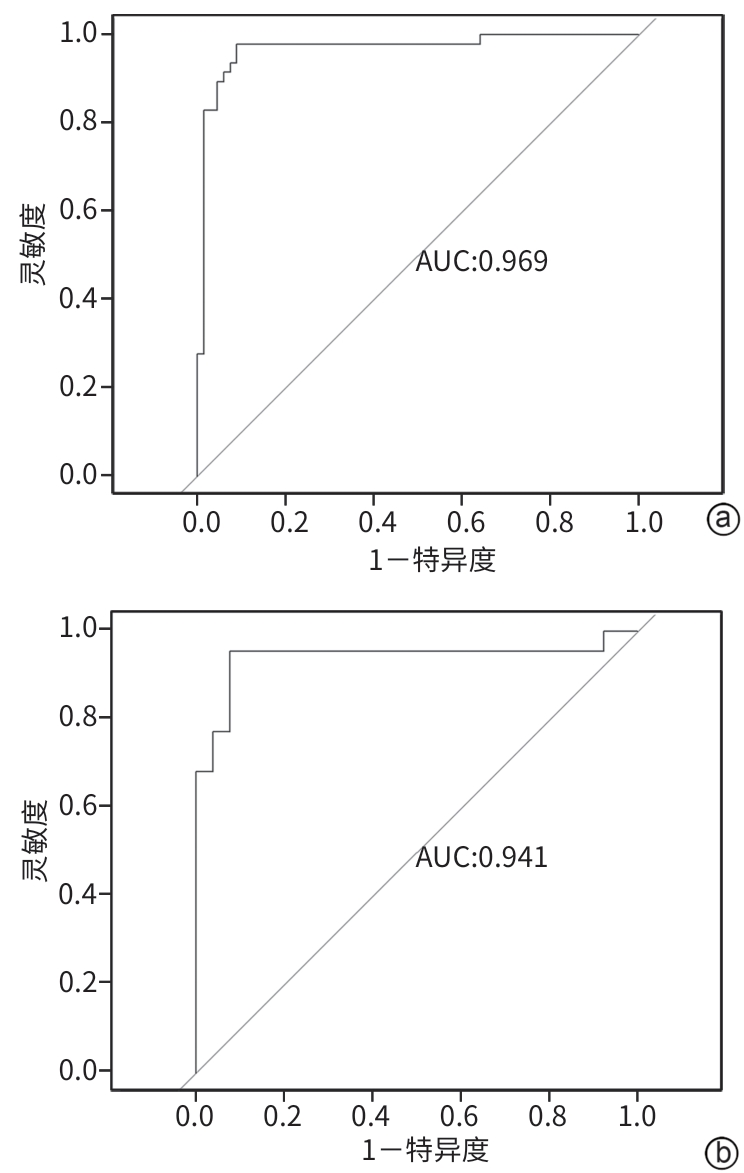
注: a,训练集;b,验证集。AKI,急性肾损伤;ROC曲线,受试者操作特征曲线。
图 3 肝移植术后AKI的列线图在训练集和验证集中的ROC曲线
Figure 3. The ROC curves for AKI after liver transplantation in the training set and validation set
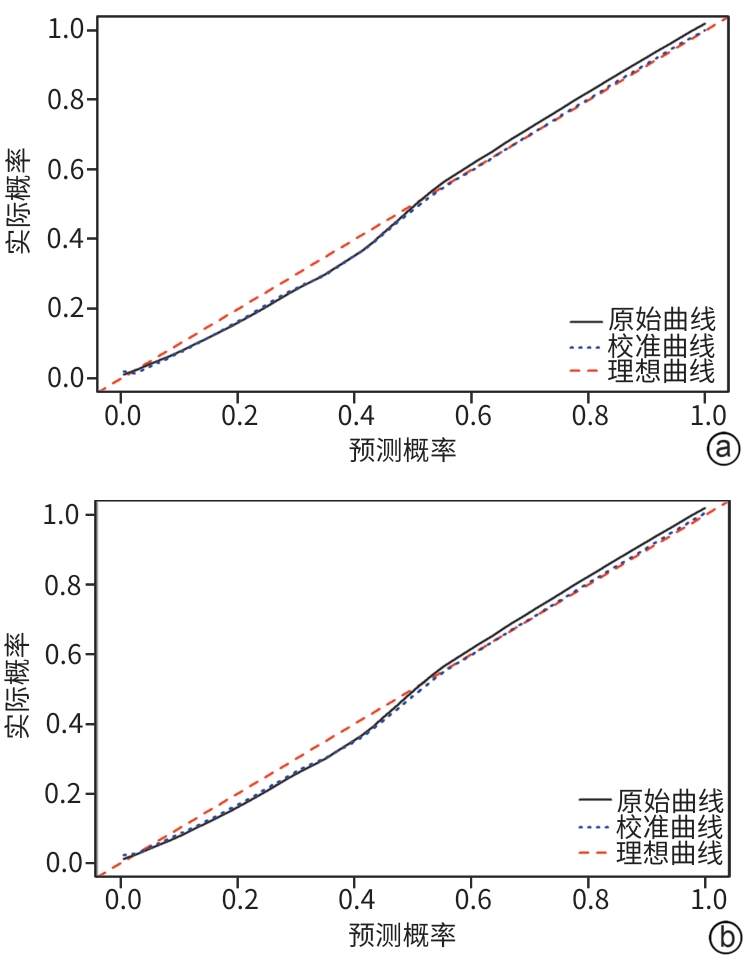
注: a,训练集;b,验证集。AKI,急性肾损伤。
图 4 肝移植术后AKI的列线图在训练集和验证集中的校准曲线
Figure 4. Calibration curves for postoperative AKI after liver transplantation in the training set and validation set
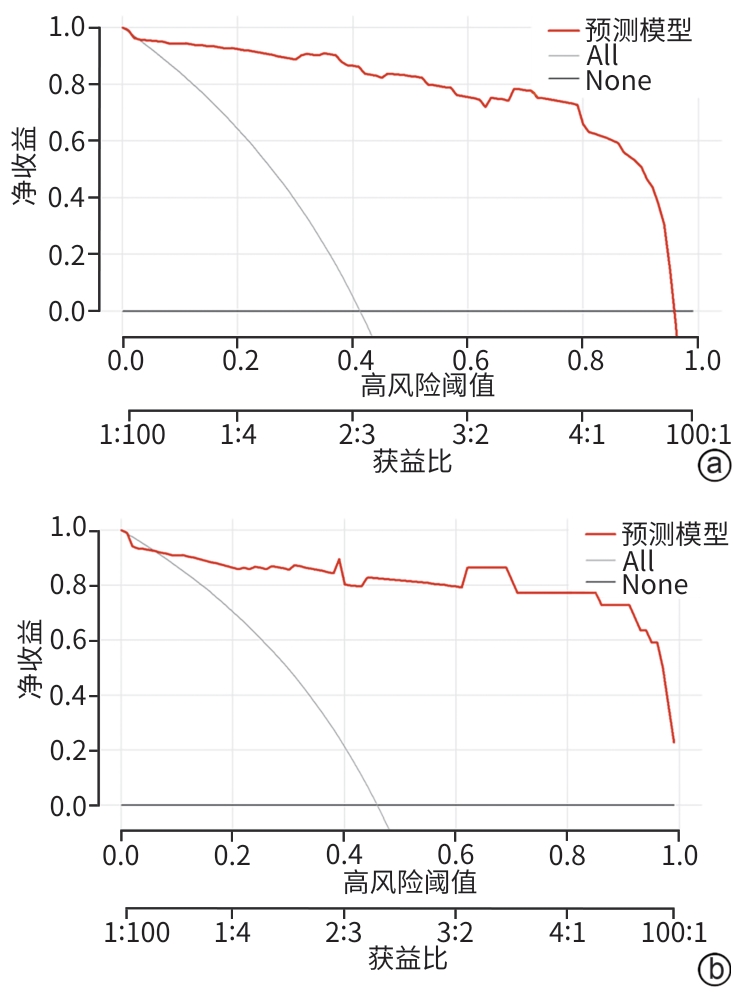
注: a,训练集;b,验证集。AKI,急性肾损伤;DCA,决策曲线分析。
图 5 肝移植术后AKI列线图预测模型的DCA
Figure 5. DCA curve analysis of the prediction model for postoperative AKI in liver transplantation
表 1 肝移植术后AKI的单因素分析
Table 1. Univariate analysis of AKI after liver transplantation
指标 总计(n=162) AKI组(n=69) 非AKI组(n=93) 统计值 P值 性别[例(%)] χ2=0.146 0.702 男 122(75.3) 53(76.8) 69(74.2) 女 40(24.6) 16(23.2) 24(25.8) 年龄[例(%)] χ2=0.463 0.496 <60岁 124(76.5) 51(74.0) 73(78.5) ≥60岁 38(23.5) 18(26.0) 20(21.5) BMI(kg/m2) 24.07±4.19 25.89±4.49 22.71±3.37 t=-5.141 <0.001 原发疾病类型[例(%)] χ2=7.452 0.114 免疫性 28(17.2) 12(17.4) 16(17.2) 肿瘤性 29(17.9) 8(11.6) 21(22.6) 病毒性 67(41.4) 36(52.2) 31(33.3) 酒精性 24(14.9) 9(13.0) 15(16.1) 其他 14(8.6) 4(5.8) 10(10.8) 肝性脑病[例(%)] 26(16) 16(23.2) 10(10.8) χ2=4.546 0.033 糖尿病[例(%)] 30(18.5) 15(21.7) 15(16.1) χ2=0.826 0.363 高血压[例(%)] 27(16.7) 12(17.4) 15(16.1) χ2=0.045 0.831 吸烟史[例(%)] 59(36.4) 23(33.3) 36(38.7) χ2=0.494 0.482 饮酒史[例(%)] 60(37.0) 24(34.8) 36(38.7) χ2=0.262 0.609 RBC(×1012/L) 3.30(2.63~3.81) 2.97(2.46~3.66) 3.38(2.86~3.94) Z=-1.734 0.083 WBC(×109/L) 3.22(2.20~5.10) 3.30(2.30~5.40) 3.00(2.20~4.90) Z=-0.552 0.581 PLT(×109/L) 54.00(37.50~89.25) 52.00(38.00~75.50) 57.00(36.00~94.00) Z=-0.654 0.513 HGB(g/L) 97.50(82.00~114.25) 94.00(78.50~107.00) 102.00(85.00~117.00) Z=-2.451 0.014 SCr(μmol/L) 62.20(52.00~77.00) 73.20(62.00~88.65) 56.20(47.50~66.75) Z=-5.733 <0.001 TBil(μmol/L) 48.30(29.85~93.23) 51.90(33.95~141.30) 44.20(22.75~81.10) Z=-1.567 0.117 DBil(μmol/L) 20.55(9.53~50.23) 24.10(11.80~57.30) 20.00(6.75~47.85) Z=-1.482 0.138 TP(g/L) 57.30(44.44~66.53) 54.10(37.65~63.65) 59.20(50.45~67.40) Z=-2.124 0.034 AST(U/L) 38.00(28.00~59.25) 38.00(28.50~55.00) 38.00(27.50~61.00) Z=-0.320 0.749 ALT(U/L) 27.00(18.00~46.25) 25.00(18.00~40.00) 28.00(18.00~47.50) Z=-0.622 0.534 PT(s) 18.25(15.80~20.93) 18.60(16.10~21.60) 17.80(15.60~20.50) Z=-1.414 0.157 APTT(s) 36.75(32.58~45.43) 39.80(33.00~50.70) 35.20(32.30~40.70) Z=-2.358 0.018 INR 1.55(1.30~1.87) 1.63(1.34~1.91) 1.47(1.27~1.84) Z=-1.846 0.065 无肝期时间(min) 55(40~67) 67(42~67) 50(40~67) Z=-1.492 0.136 冷缺血时间(min) 180(170~210) 185(180~360) 180(165~185) Z=-5.282 <0.001 供肝血供恢复-胆道吻合时间(min) 40(40~60) 40(40~60) 40(10~250) Z=-0.982 0.326 无肝期尿量(min) 200(60~500) 500(55~500) 150(65.5~500) Z=-0.499 0.618 术中输注红细胞(mL) 12(8~18) 14(10~18) 12(8~18) Z=-1.463 0.143 术中输注血浆(mL) 1 000(0~2 000) 1 000(0~1 900) 1 000(0~2 000) Z=-0.565 0.572 术中出血量(mL) 1 000(800~1 200) 1 200(1 050~1 500) 800(650~1 000) Z=-8.465 <0.001 术后AST峰值(U/L) 862.50(371.25~1 454.75) 986.00(370.00~1 893.50) 804.00(369.50~1 209.50) Z=-1.501 0.133 术后ALT峰值(U/L) 493.00(269.00~737.50) 531.00(263.50~846.00) 422.00(274.00~657.50) Z=-1.501 0.133 术后感染[例(%)] 40(24.7) 29(42.0) 11(11.8) χ2=19.430 <0.001 术后使用万古霉素[例(%)] 28(17.3) 14(20.3) 14(15.1) χ2=0.760 0.383 注:AKI,急性肾损伤;BMI,体重指数;RBC,红细胞;WBC,白细胞;PLT,血小板;HGB,血红蛋白;SCr,血肌酐;TBil,总胆红素;DBil,直接胆红素;TP,总蛋白;AST,天冬氨酸氨基转移酶;ALT,丙氨酸氨基转移酶;PT,凝血酶原时间;APTT,活化部分凝血活酶时间;INR,国际标准化比值。
 下载: 导出CSV
下载: 导出CSV
表 2 肝移植术后AKI的多因素Logistic分析
Table 2. Multivariate Logistic analysis of AKI after liver transplantation
变量 β值 SE Wald P值 OR 95%CI BMI 0.248 0.108 5.278 0.022 1.281 1.037~1.582 肝性脑病 1.435 0.805 3.180 0.075 4.200 0.867~20.33 HGB -0.001 0.004 0.109 0.742 0.999 0.992~1.006 APTT 0.007 0.046 0.024 0.876 1.007 0.921~1.101 SCr 0.093 0.037 6.159 0.013 1.097 1.020~1.181 TP -0.032 0.040 0.657 0.418 0.968 0.896~1.047 冷缺血时间 -0.016 0.004 18.067 <0.001 0.984 0.976~0.991 术中出血量 0.005 0.002 8.273 0.004 1.005 1.002~1.009 术后感染 -1.058 1.797 21.347 0.055 0.347 0.118~1.023 注:AKI,急性肾损伤;BMI,体重指数;HGB,血红蛋白;APTT,活化部分凝血活酶时间;SCr,血肌酐;TP,总蛋白;OR,比值比;CI,置信区间。
下载: 导出CSV
-
[1] AGOSTINI C, BUCCIANTI S, RISALITI M, et al. Complications in post-liver transplant patients[J]. J Clin Med, 2023, 12( 19): 6173. DOI: 10.3390/jcm12196173. [2] TERRAULT NA, FRANCOZ C, BERENGUER M, et al. Liver transplantation 2023: Status report, current and future challenges[J]. Clin Gastroenterol Hepatol, 2023, 21( 8): 2150- 2166. DOI: 10.1016/j.cgh.2023.04.005. [3] CHEN PF, CHEN MJ, CHEN L, et al. Risk factors for severe acute kidney injury post complication after total arch replacement combined with frozen elephant trunk, in acute type A aortic dissection[J]. Cardiovasc Diagn Ther, 2022, 12( 6): 880- 891. DOI: 10.21037/cdt-22-313. [4] LUO CC, ZHONG YL, QIAO ZY, et al. Development and validation of a nomogram for postoperative severe acute kidney injury in acute type A aortic dissection[J]. J Geriatr Cardiol, 2022, 19( 10): 734- 742. DOI: 10.11909/j.issn.1671-5411.2022.10.003. [5] WANG ZG, GE M, WANG ZY, et al. Identification of risk factors for postoperative stage 3 acute kidney injury in patients who received surgical repair for acute type A aortic dissection[J]. BMC Surg, 2022, 22( 1): 75. DOI: 10.1186/s12893-022-01526-x. [6] HUANG JY, CHEN JJ, YANG J, et al. Prediction models for acute kidney injury following liver transplantation: A systematic review and critical appraisal[J]. Intensive Crit Care Nurs, 2025, 86: 103808. DOI: 10.1016/j.iccn.2024.103808. [7] SAKAI T. Acute kidney injury after adult liver transplantation-Doesn't intraoperative management matter?[J]. Liver Transpl, 2022, 28( 7): 1131- 1132. DOI: 10.1002/lt.26469. [8] KHWAJA A. KDIGO clinical practice guidelines for acute kidney injury[J]. Nephron Clin Pract, 2012, 120( 4): c179- c184. DOI: 10.1159/000339789. [9] PIOVANI D, SOKOU R, TSANTES AG, et al. Optimizing clinical decision making with decision curve analysis: Insights for clinical investigators[J]. Healthcare, 2023, 11( 16): 2244. DOI: 10.3390/healthcare11162244. [10] KALISVAART M, SCHLEGEL A, UMBRO I, et al. The impact of combined warm ischemia time on development of acute kidney injury in donation after circulatory death liver transplantation: Stay within the golden hour[J]. Transplantation, 2018, 102( 5): 783- 793. DOI: 10.1097/TP.0000000000002085. [11] THONGPRAYOON C, KAEWPUT W, THAMCHAROEN N, et al. Incidence and impact of acute kidney injury after liver transplantation: A meta-analysis[J]. J Clin Med, 2019, 8( 3): 372. DOI: 10.3390/jcm8030372. [12] DURAND F, FRANCOZ C, ASRANI SK, et al. Acute kidney injury after liver transplantation[J]. Transplantation, 2018, 102( 10): 1636- 1649. DOI: 10.1097/TP.0000000000002305. [13] THANAPONGSATORN P, CHAIKOMON K, LUMLERTGUL N, et al. Comprehensive versus standard care in post-severe acute kidney injury survivors, a randomized controlled trial[J]. Crit Care, 2021, 25( 1): 322. DOI: 10.1186/s13054-021-03747-7. [14] KOLLMANN D, NEONG SF, ROSALES R, et al. Renal dysfunction after liver transplantation: Effect of donor type[J]. Liver Transpl, 2020, 26( 6): 799- 810. DOI: 10.1002/lt.25755. [15] de HAAN JE, HOORN EJ, de GEUS HRH. Acute kidney injury after liver transplantation: Recent insights and future perspectives[J]. Best Pract Res Clin Gastroenterol, 2017, 31( 2): 161- 169. DOI: 10.1016/j.bpg.2017.03.004. [16] PACHECO MP, CARNEIRO-D'ALBUQUERQUE LA, MAZO DF. Current aspects of renal dysfunction after liver transplantation[J]. World J Hepatol, 2022, 14( 1): 45- 61. DOI: 10.4254/wjh.v14.i1.45. [17] GUO DD, WANG HF, LAI XY, et al. Development and validation of a nomogram for predicting acute kidney injury after orthotopic liver transplantation[J]. Ren Fail, 2021, 43( 1): 1588- 1600. DOI: 10.1080/0886022X.2021.2009863. [18] ZHANG DL, LIU ZW, BI JF, et al. Risk factors for the incidence and severity of acute kidney injury after liver transplantation[J]. Turk J Gastroenterol, 2021, 32( 1): 82- 87. DOI: 10.5152/tjg.2020.19592. [19] OH J, RABB H. Adiponectin: An enlarging role in acute kidney injury[J]. Kidney Int, 2013, 83( 4): 546- 548. DOI: 10.1038/ki.2012.479. [20] TARGHER G, CHONCHOL M, ZOPPINI G, et al. Risk of chronic kidney disease in patients with non-alcoholic fatty liver disease: Is there a link?[J]. J Hepatol, 2011, 54( 5): 1020- 1029. DOI: 10.1016/j.jhep.2010.11.007. [21] RAJA K, PANACKEL C. Post liver transplant renal dysfunction-evaluation, management and immunosuppressive practice[J]. J Clin Exp Hepatol, 2024, 14( 2): 101306. DOI: 10.1016/j.jceh.2023.101306. [22] WU ZP, WANG Y, HE L, et al. Development of a nomogram for the prediction of acute kidney injury after liver transplantation: A model based on clinical parameters and postoperative cystatin C level[J]. Ann Med, 2023, 55( 2): 2259410. DOI: 10.1080/07853890.2023.2259410. [23] ZHANG YH, YANG D, LIU ZF, et al. An explainable supervised machine learning predictor of acute kidney injury after adult deceased donor liver transplantation[J]. J Transl Med, 2021, 19( 1): 321. DOI: 10.1186/s12967-021-02990-4. [24] CATALÁN R, JIMÉNEZ-CEJA JV, RINCÓN-PEDRERO R, et al. Factors associated with development of acute kidney injury after liver transplantation[J]. Rev Invest Clin, 2022, 74( 2): 090- 096. DOI: 10.24875/RIC.21000496. [25] HIZOMI ARANI R, ABBASI MR, MANSOURNIA MA, et al. Acute kidney injury after liver transplant: Incidence, risk factors, and impact on patient outcomes[J]. Exp Clin Transplant, 2021, 19( 12): 1277- 1285. DOI: 10.6002/ect.2021.0300. [26] MOURA AF, MOURA-NETO JA, DE MELO RIBEIRO B, et al. Post-liver transplant kidney dysfunction: Incidence of acute kidney injury and chronic kidney disease and risk factors related to chronic kidney disease development[J]. Diseases, 2025, 13( 5): 144. DOI: 10.3390/diseases13050144. [27] ZHAO Q, HUANG JB, QIN MT, et al. Protective value of ischemia-free liver transplantation on post-transplant acute kidney injury[J]. JHEP Rep, 2025, 7( 4): 101339. DOI: 10.1016/j.jhepr.2025.101339. [28] GONG XY, DU GS, LI HP, et al. Analysis of risk factors for acute kidney injury after liver transplantation[J]. Chin J Med Offic, 2025, 53( 12): 1303- 1305, 1309. DOI: 10.16680/j.1671-3826.2025.12.25.宫学宇, 杜国盛, 李怀朋, 等. 肝移植术后发生急性肾损伤危险因素分析[J]. 临床军医杂志, 2025, 53( 12): 1303- 1305, 1309. DOI: 10.16680/j.1671-3826.2025.12.25. [29] CHIU PF, LIN PR, TSAI CC, et al. The impact of acute kidney injury with or without recovery on long-term kidney outcome in patients undergoing living liver transplantation[J]. Nephrol Dial Transplant, 2023, 38( 8): 1817- 1822. DOI: 10.1093/ndt/gfad005. -

 本文二维码
本文二维码
计量
- 文章访问数: 246
- HTML全文浏览量: 199
- PDF下载量: 97
- 被引次数: 0

