
 PDF下载 ( 8936 KB)
PDF下载 ( 8936 KB)

基于2021年全球疾病负担数据库的中国肝母细胞瘤疾病负担分析
DOI: 10.12449/JCH251218
Disease burden analysis of hepatoblastoma in China based on the 2021 global burden of disease database
-
摘要:
目的 分析1990—2021年中国肝母细胞瘤(HB)疾病负担的时空变化特点并进行未来预测,研究疾病负担与社会经济因素的相关性。 方法 从2021年全球疾病负担数据库(GBD)获取1990 — 2021年中国HB的疾病负担数据:发病、死亡、伤残调整生命年(DALY)的绝对数和年龄标准化率;利用Joinpoint回归模型分析疾病负担情况的时间变化趋势,构建年龄-时期-队列(APC)模型解析驱动疾病负担变化的3个主要因素的贡献情况,通过健康不平等分析研究疾病负担情况与社会人口学指数(SDI)的关系,构建自回归积分滑动平均模型和贝叶斯年龄周期模型对HB的疾病负担进行未来预测。 结果 1990—2021年中国HB疾病负担显著下降,发病数减少75.62%(全球减少42.69%),死亡数下降86.26%(全球下降49.96%),DALY降低86.32%(全球降低49.93%)。疾病的年龄标准化发病率(ASIR)、年龄标准化死亡率(ASMR)、年龄标准化伤残调整生命年率[AS(DALY)R]均下降,分别降低3.90%、4.44%、5.93%,下降程度均高于全球水平(2.03%、2.19%、2.73%)。APC模型显示年龄效应(25.17%)和流行病趋势(87.46%)是主要驱动因素,SDI与疾病负担呈非线性相关。预测模型显示2021年后ASIR将持续下降,ASMR和AS(DALY)R将保持稳定。 结论 1990—2021年中国HB疾病负担呈下降趋势,年龄效应和流行病学趋势是主要驱动因素,SDI相关分析提示需关注中高发展水平地区的防控优化。预测结果表明当前防治策略具有持续效益,但需警惕特定年龄段的疾病风险。 Abstract:Objective To investigate the spatiotemporal changes of the disease burden of hepatoblastoma (HB) in China from 1990 to 2021, to predict future trends, and to analyze the correlation between disease burden and socioeconomic factors. Methods The 2021 Global Burden of Disease database was used to obtain the disease burden data of HB in China in 1990 — 2021, including the absolute numbers and age-standardized rates of incidence, mortality, and disability-adjusted life years (DALY). The Joinpoint regression model was used to analyze the temporal trends in disease burden, and an age-period-cohort (APC) model was constructed to investigate the contribution of three main factors driving the changes in disease burden. Health inequality analysis was used to investigate the correlation between disease burden and the socio-demographic index (SDI), and Autoregressive Integrated Moving Average and Bayesian Age-Period-Cohort models were established to predict the future disease burden of HB. Results There was a significant reduction in the disease burden of HB in China from 1990 to 2021, and the numbers of incidence, mortality, and DALY were reduced by 75.62% (42.69% globally), 86.26% (49.96% globally), and 86.32% (49.93% globally), respectively. The age-standardized incidence rate (ASIR), age-standardized mortality rate (ASMR), and age-standardized DALY rate [AS(DALY)R] of the disease were reduced by 3.90%, 4.44%, and 5.93%, respectively, with greater reductions than the global levels (2.03%, 2.19%, and 2.73%, respectively). The APC model showed that age effect (25.17%) and epidemiological trend (87.46%) were the main driving factors, and nonlinear correlation was observed between SDI and disease burden. Predictive models showed that ASIR would continue to decline after 2021, while ASMR and AS(DALY)R would remain stable. Conclusion There was a tendency of reduction in the disease burden of HB in China in 1990 — 2021, with age effect and epidemiological trend as the main driving factors, and the SDI correlation analysis shows that it is needed to focus on the optimization of prevention and control in regions with medium to high levels of development. Prediction results indicate the sustained effectiveness of current prevention and control strategies, but the risk of diseases in specific age groups should be closely monitored. -
Key words:
- Hepatoblastoma /
- Cost of Illness /
- Epidemiologic Studies
-
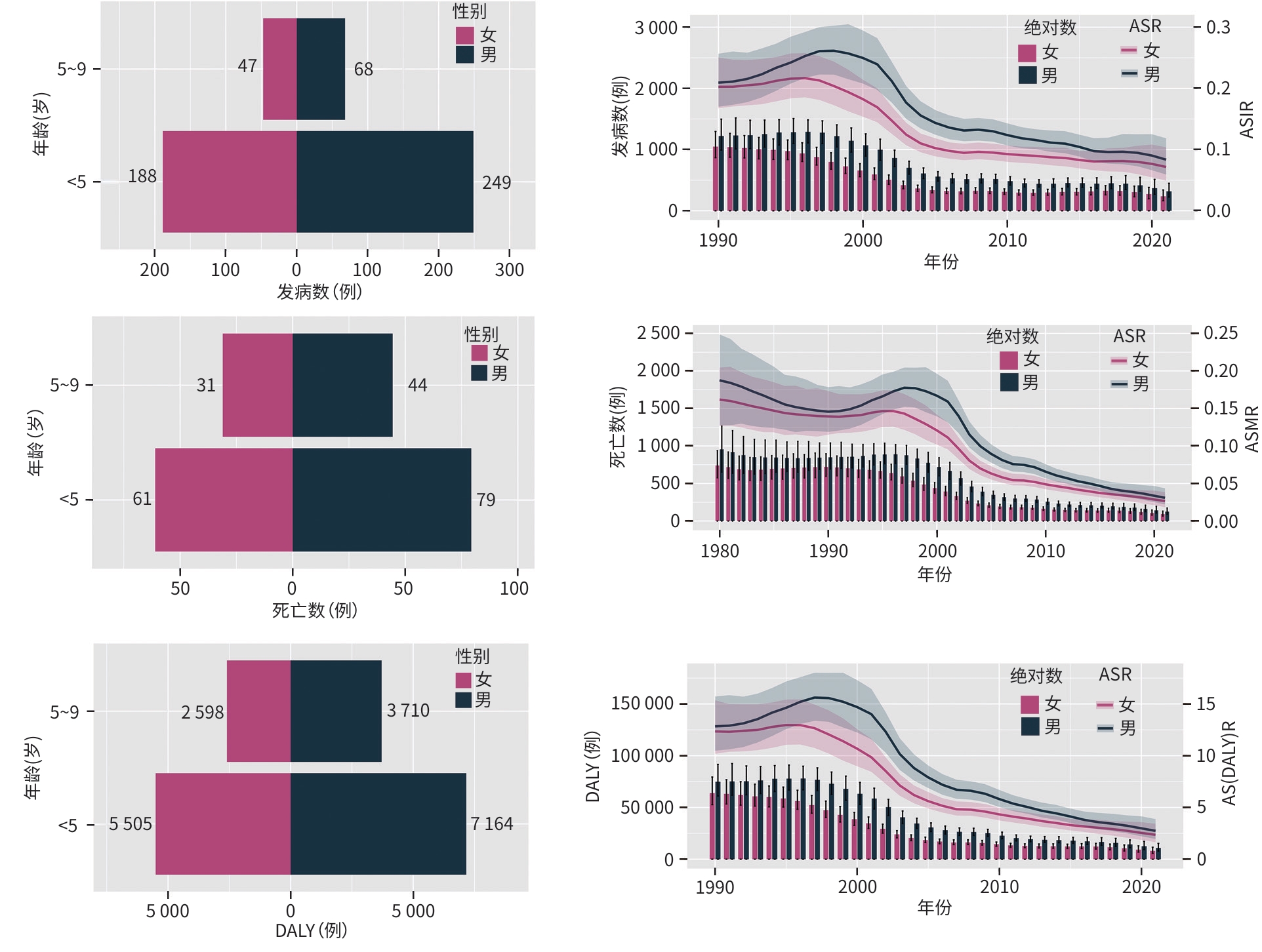
注: ASR,年龄标准化率;ASIR,年龄标准化发病率;ASMR,年龄标准化死亡率;AS(DALY)R,年龄标准化伤残调整生命年率。
图 1 2021年中国HB的发病、死亡、DALY情况及1990—2021年的变化趋势
Figure 1. The incidence, mortality, and DALY of HB in China in 2021 and the changing trends from 1990 to 2021

注: ASIR,年龄标准化发病率;ASMR,年龄标准化死亡率;AS(DALY)R,年龄标准化伤残调整生命年率。*P<0.05。
图 2 1990—2021年中国HB疾病负担ASR的Joinpoint回归分析
Figure 2. Joinpoint regression analysis of ASR for HB disease burden in China from 1990 to 2021
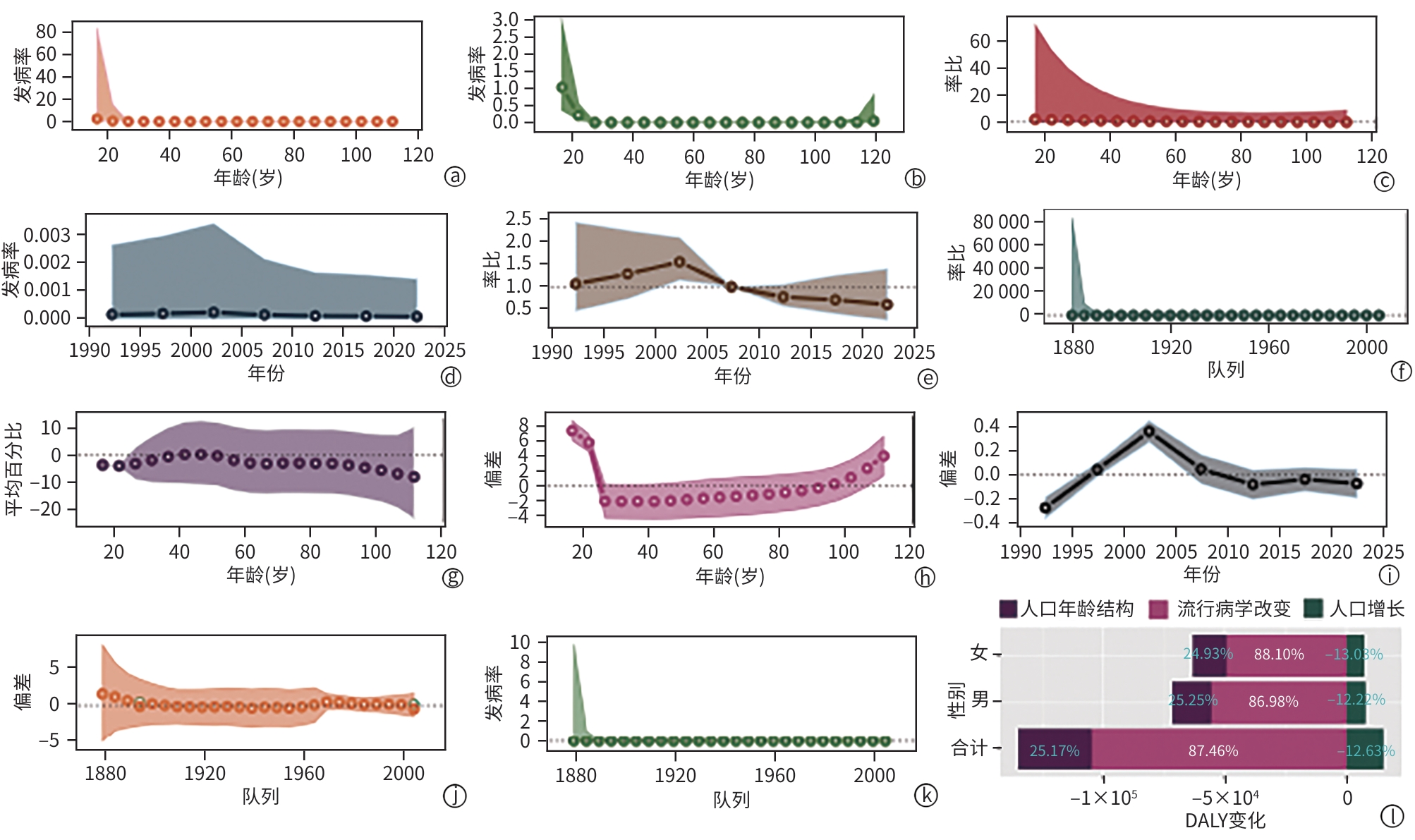
注: a,纵向年龄曲线:展示不同年龄段的发病率随时间变化的趋势;b,横截面年龄曲线:显示单个时间点不同年龄组的发病率;c,纵向与横截面相对风险的对比:显示两种方法计算的风险比的一致性;d,拟合的时间趋势:揭示1990—2025年发病率的变化;e,周期相对风险:展示不同时间段的风险变化;f,队列相对风险:分析不同出生队列的风险差异;g,局部漂移:描述每年每年龄组的百分比变化;h,年龄偏差:评估发病率偏离整体趋势的程度;i,时间偏差:分析时间段对发病率的影响;j,队列偏差:评估不同出生队列的发病率偏离程度;k,拟合队列模式:揭示出生队列对发病率的长期影响;l,HB疾病负担的分解分析:研究人口年龄结构、人口增长和流行病学改变3个因素对于DALY变化的贡献权重。DALY,伤残调整生命年。
图 3 中国HB疾病负担的APC模型和分解分析
Figure 3. APC model and decomposition analysis of HB disease burden in China

注: ASR,年龄标准化率;DALY,伤残调整生命年;SDI,社会人口学指数;SII,不平等斜率指数;CI,集中指数。
图 4 HB疾病负担与SDI的相关性和健康不平等分析
Figure 4. Correlation analysis of HB disease burden with SDI and health inequality analysis
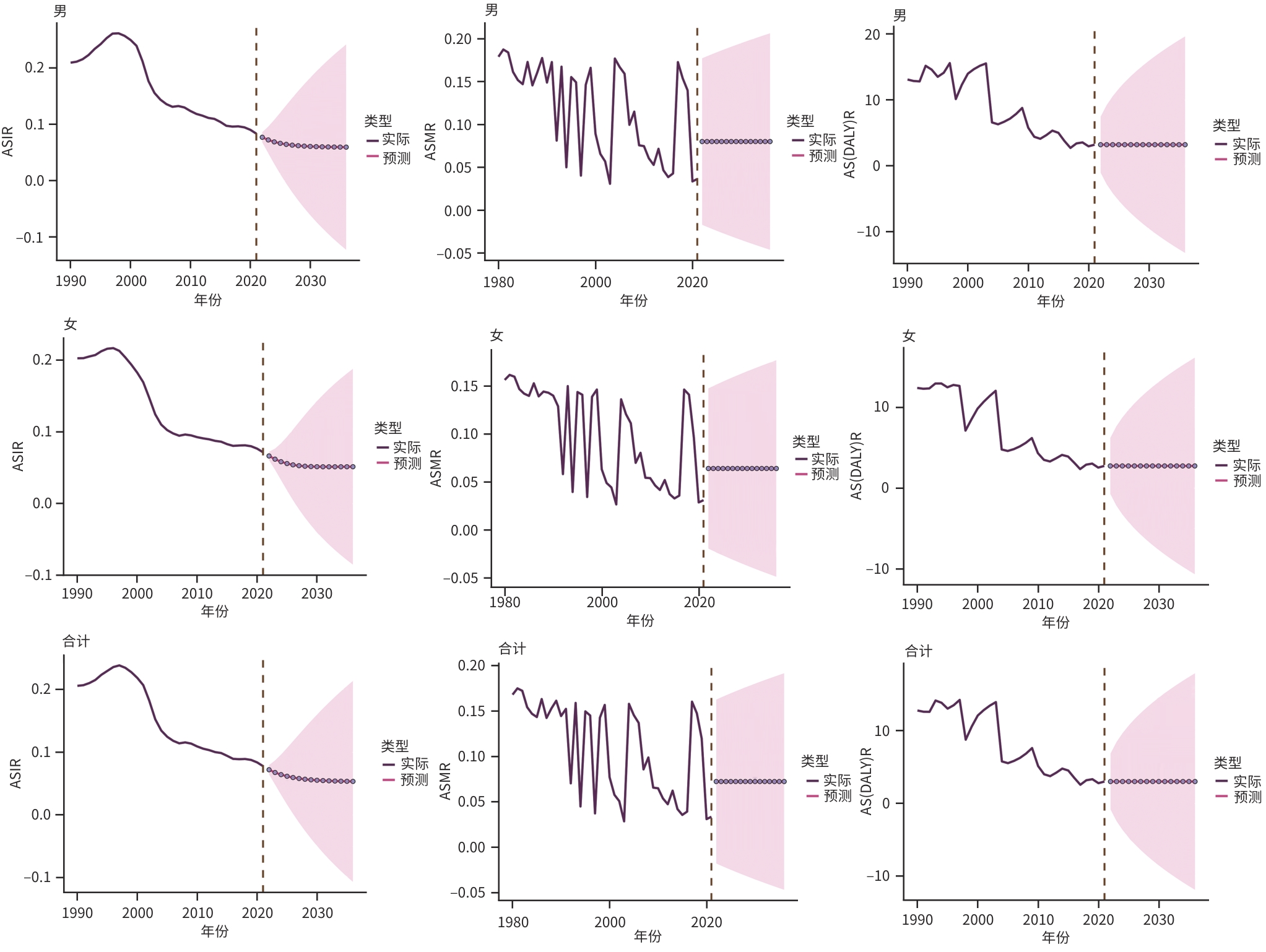
注: ASIR,年龄标准化发病率;ASMR,年龄标准化死亡率;AS(DALY)R,年龄标准化伤残调整生命年率。
图 5 ARIMA模型对中国HB疾病负担的未来预测
Figure 5. ARIMA model-based prediction of future HB disease burden in China
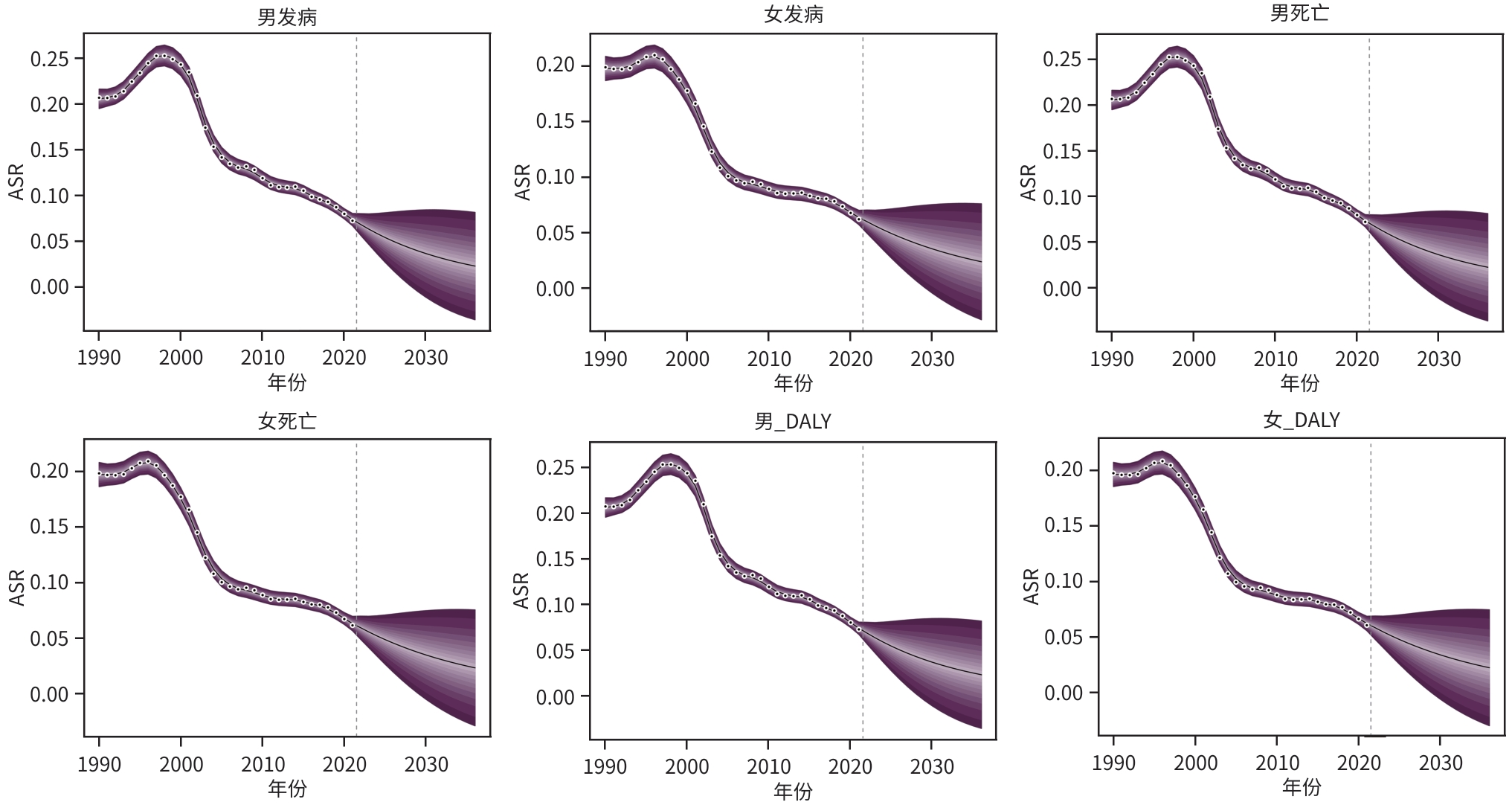
注: ASR,年龄标准化率;DALY,死亡和伤残调整生命年。
图 6 BAPC模型对中国HE疾病负担的未来预测
Figure 6. BAPC model-based prediction of future HE disease burden in China
表 1 1990—2021年中国HB的发病、死亡、DALY情况
Table 1. Incidence, mortality, and DALY for HB in China from 1990 to 2021
指标 地区 性别 1990年(95%UI) 2021年(95%UI) 变化百分比(95%UI) 发病数(例) 中国 男 1 221(992~1 497) 317(224~448) -74.04% (-85.02%~-54.80%) 女 1 048(867~1 296) 236(163~340) -77.47% (-87.41%~-60.85%) 合计 2 269(1 881~2 784) 553(391~783) -75.62% (-85.96%~-58.35%) 全球 男 3 735(3 028~4 344) 2 088(1 699~2 558) -44.10% (-60.90%~-15.52%) 女 3 328(2 657~4 001) 1 960(1 541~2 500) -41.10% (-61.48%~-5.93%) 合计 7 064(5 799~8 281) 4 048(3 252~5 000) -42.69% (-60.72%~-13.77%) 死亡数(例) 中国 男 849(692~1040) 124(89~173) -85.43% (-91.45%~-75.00%) 女 721(596~896) 92(65~132) -87.23% (-92.77%~-77.86%) 合计 1 570(1 305~1 924) 216(155~302) -86.26% (-91.95%~-76.88%) 全球 男 2 548(2 050~2 972) 1 219(980~1520) -52.18% (-67.04%~-25.89%) 女 2 280(1 811~2 761) 1 198(929~1537) -47.48% (-66.34%~-15.10%) 合计 4 828(3 939~5 671) 2 416(1 922~3 019) -49.96% (-66.10%~-23.35%) DALY(例) 中国 男 74 837(61 110~91 628) 10 874(7 801~15 250) -85.47%(-91.49%~-75.05%) 女 63 880(52 688~79 391) 8 104(5 687~11 586) -87.31%(-92.84%~-78.01%) 合计 138 716(115 370~169 802) 18 978(13 614~26 641) -86.32%(-91.98%~-76.91%) 全球 男 224 735 (181 064~263 142) 107 615(86 429~134 376) -52.11% (-67.15%~-25.79%) 女 201 630 (160 044~244 339) 105 863(82 258~135 574) -47.50% (-66.33%~-15.29%) 合计 426 365 (348 856~500 156) 213 478(170 090~267 250) -49.93% (-65.99%~-23.39%) 注:DALY,伤残调整生命年;UI,不确定性区间,用于描述单个点估计的不确定性,GBD研究的特有指标。
 下载: 导出CSV
下载: 导出CSV
表 2 1990—2021年中国HB的ASIR、ASMR、AS(DALY)R
Table 2. Age-standardized incidence rate, mortality rate, DALY rate of HB in China from 1990 to 2021
指标 地区 性别 1990年(95%UI) 2021年(95%UI) EAPC(95%CI) ASIR 中国 男 0.21 (0.17~0.26) 0.08 (0.06~0.12) -3.78%(-4.31%~-3.24%) 女 0.20 (0.17~0.25) 0.07 (0.05~0.10) -4.07%(-4.55%~-3.57%) 合计 0.21 (0.17~0.25) 0.08 (0.06~0.11) -3.90%(-4.38%~-3.42%) 全球 男 0.12 (0.09~0.14) 0.06 (0.05~0.08) -2.16%(-2.32%~-2.00%) 女 0.11 (0.09~0.13) 0.06 (0.05~0.08) -1.89%(-2.03%~-1.74%) 合计 0.11 (0.09~0.13) 0.06 (0.05~0.08) -2.03%(-2.17%~-1.89%) ASMR 中国 男 0.15 (0.12~0.18) 0.03 (0.02~0.04) -4.27%(-4.87%~-3.68%) 女 0.14 (0.12~0.17) 0.03 (0.02~0.04) -4.68%(-5.16%~-4.19%) 合计 0.14 (0.12~0.17) 0.03 (0.02~0.04) -4.44%(-4.98%~-3.89%) 全球 男 0.08 (0.06~0.09) 0.04 (0.03~0.04) -2.32%(-2.48%~-2.17%) 女 0.08 (0.06~0.09) 0.04 (0.03~0.05) -2.04%(-2.15%~-1.93%) 合计 0.08 (0.06~0.09) 0.04 (0.03~0.05) -2.19%(-2.32%~-2.06%) AS(DALY)R 中国 男 12.84 (10.49~15.71) 2.74 (1.96~3.87) -5.83%(-6.49%~-5.17%) 女 12.35 (10.19~15.35) 2.36 (1.65~3.42) -6.07%(-6.53%~-5.60%) 合计 12.60 (10.48~15.42) 2.56 (1.83~3.63) -5.93%(-6.49%~-5.37%) 全球 男 7.05 (5.68~8.26) 3.19 (2.56~3.97) -2.73%(-2.90%~-2.57%) 女 6.73 (5.34~8.16) 3.36 (2.61~4.31) -2.30%(-2.43%~-2.17%) 合计 6.90 (5.64~8.09) 3.27 (2.61~4.10) -2.73%(-2.90%~-2.57%) 注:ASIR,年龄标准化发病率;ASMR,年龄标准化死亡率;AS(DALY)R,年龄标准化伤残调整生命年率;UI,不确定性区间;EAPC,年度百分比变化估计值;95%CI,95%置信区间。
下载: 导出CSV
-
[1] SHARMA D, SUBBARAO G, SAXENA R. Hepatoblastoma[J]. Semin Diagn Pathol, 2017, 34( 2): 192- 200. DOI: 10.1053/j.semdp.2016.12.015. [2] GUO CN, LIU ZQ, ZHANG X, et al. Global, regional, and national epidemiology of hepatoblastoma in children from 1990 to 2021: A trend analysis[J]. Hepatol Int, 2025, 19( 1): 156- 165. DOI: 10.1007/s12072-024-10750-x. [3] TANG MJ, MA XL, HE XL, et al. A multicenter prospective study on the management of hepatoblastoma in children: A report from the Chinese Children's Cancer Group[J]. World J Pediatr, 2024, 20( 6): 590- 601. DOI: 10.1007/s12519-023-00750-6. [4] GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: A systematic analysis for the Global Burden of Disease Study 2021[J]. Lancet, 2024, 403( 10440): 2100- 2132. DOI: 10.1016/S0140-6736(24)00367-2. [5] ZENG SQ. Joinpoint regression model and its application in epidemic trend analysis of infectious diseases[J]. Chin J Health Stat, 2019, 36( 5): 787- 791.曾四清. Joinpoint回归模型及其在传染病流行趋势分析中的应用[J]. 中国卫生统计, 2019, 36( 5): 787- 791. [6] ROSENBERG PS, MIRANDA-FILHO A, WHITEMAN DC. Comparative age-period-cohort analysis[J]. BMC Med Res Methodol, 2023, 23( 1): 238. DOI: 10.1186/s12874-023-02039-8. [7] KNOLL M, FURKEL J, DEBUS J, et al. An R package for an integrated evaluation of statistical approaches to cancer incidence projection[J]. BMC Med Res Methodol, 2020, 20( 1): 257. DOI: 10.1186/s12874-020-01133-5. [8] LU YF, WANG BB, WANG Y. Progress in nursing research for children with hepatoblastoma after liver transplantation[J/OL]. Chin J Transplatation Electron Ed, 2024, 18( 6): 412- 416. DOI: 10.3877/cma.j.issn.1674-3903.2024.06.011.陆晔峰, 王贝贝, 王艳. 肝母细胞瘤患儿移植护理研究进展[J/OL]. 中华移植杂志(电子版), 2024, 18( 6): 412- 416. DOI: 10.3877/cma.j.issn.1674-3903.2024.06.011. [9] FENG JC, POLYCHRONIDIS G, HEGER U, et al. Incidence trends and survival prediction of hepatoblastoma in children: A population-based study[J]. Cancer Commun, 2019, 39( 1): 62. DOI: 10.1186/s40880-019-0411-7. [10] ZHU LR, ZHENG WQ, GAO Q, et al. Epigenetics and genetics of hepatoblastoma: Linkage and treatment[J]. Front Genet, 2022, 13: 1070971. DOI: 10.3389/fgene.2022.1070971. [11] CAO YB, WU SR, TANG HW. An update on diagnosis and treatment of hepatoblastoma[J]. Biosci Trends, 2024, 17( 6): 445- 457. DOI: 10.5582/bst.2023.01311. [12] Compilation and Examination Expert Group for Guidelines for the diagnosis and treatment of hepatoblastoma(2019). Guidelines for the diagnosis and treatment of hepatoblastoma(2019)[J]. J Clin Hepatol, 2019, 35( 11): 2431- 2434. DOI: 10.3969/j.issn.1001-5256.2019.11.008.儿童肝母细胞瘤诊疗规范(2019年版)编写审定专家组. 儿童肝母细胞瘤诊疗规范(2019年版)[J]. 临床肝胆病杂志, 2019, 35( 11): 2431- 2434. DOI: 10.3969/j.issn.1001-5256.2019.11.008. [13] ZHEN ZJ, LIU JC, ZHOU L, et al. Treatment outcome of 100 patients with hepatoblastoma based on a new risk stratification[J]. Chin J Oncol, 2021, 43( 2): 228- 232. DOI: 10.3760/cma.j.cn112152-20190603-00347.甄子俊, 刘钧澄, 周李, 等. 100例肝母细胞瘤基于新危险分层的治疗结果分析[J]. 中华肿瘤杂志, 2021, 43( 2): 228- 232. DOI: 10.3760/cma.j.cn112152-20190603-00347. [14] MEYERS RL, MAIBACH R, HIYAMA E, et al. Risk-stratified staging in paediatric hepatoblastoma: A unified analysis from the Children’s hepatic tumors international collaboration[J]. Lancet Oncol, 2017, 18( 1): 122- 131. DOI: 10.1016/S1470-2045(16)30598-8. [15] HAFBERG E, BORINSTEIN SC, ALEXOPOULOS SP. Contemporary management of hepatoblastoma[J]. Curr Opin Organ Transplant, 2019, 24( 2): 113- 117. DOI: 10.1097/MOT.0000000000000618. [16] LIU J, DONG Q, XIU WL, et al. New progress of precision liver surgery in the treatment of children hepatoblastoma[J]. J Hepatopancreatobiliary Surg, 2024, 36( 12): 762- 768.刘洁, 董蒨, 修文丽, 等. 精准肝脏外科在儿童肝母细胞瘤治疗中的研究新进展[J]. 肝胆胰外科杂志, 2024, 36( 12): 762- 768. [17] KATZENSTEIN HM, LANGHAM MR, MALOGOLOWKIN MH, et al. Minimal adjuvant chemotherapy for children with hepatoblastoma resected at diagnosis(AHEP0731): A Children’s Oncology Group, multicentre, phase 3 trial[J]. Lancet Oncol, 2019, 20( 5): 719- 727. DOI: 10.1016/S1470-2045(18)30895-7. [18] ZSIROS J, BRUGIERES L, BROCK P, et al. Dose-dense cisplatin-based chemotherapy and surgery for children with high-risk hepatoblastoma(SIOPEL-4): A prospective, single-arm, feasibility study[J]. Lancet Oncol, 2013, 14( 9): 834- 842. DOI: 10.1016/S1470-2045(13)70272-9. [19] DEMBOWSKA-BAGIŃSKA B, WIĘCKOWSKA J, BROŻYNA A, et al. Health status in long-term survivors of hepatoblastoma[J]. Cancers, 2019, 11( 11): 1777. DOI: 10.3390/cancers11111777. [20] WU PV, RANGASWAMI A. Current approaches in hepatoblastoma-new biological insights to inform therapy[J]. Curr Oncol Rep, 2022, 24( 9): 1209- 1218. DOI: 10.1007/s11912-022-01230-2. [21] LIANG Y, GAO HX, SHAN YH, et al. Analysis of prognostic factors in children with hepatoblastoma[J]. Chin J Clin Med, 2022, 29( 3): 338- 345.梁煜, 高鸿翔, 单禹华, 等. 儿童肝母细胞瘤预后影响因素分析[J]. 中国临床医学, 2022, 29( 3): 338- 345. [22] LUPO PJ, SCHRAW JM, DESROSIERS TA, et al. Association between birth defects and cancer risk among children and adolescents in a population-based assessment of 10 million live births[J]. JAMA Oncol, 2019, 5( 8): 1150- 1158. DOI: 10.1001/jamaoncol.2019.1215. [23] HECK JE, MEYERS TJ, LOMBARDI C, et al. Case-control study of birth characteristics and the risk of hepatoblastoma[J]. Cancer Epidemiol, 2013, 37( 4): 390- 395. DOI: 10.1016/j.canep.2013.03.004. [24] ADAWY A, KOMOHARA Y, HIBI T. Tumor-associated macrophages: The key player in hepatoblastoma microenvironment and the promising therapeutic target[J]. Microbiol Immunol, 2024, 68( 8): 249- 253. DOI: 10.1111/1348-0421.13162. [25] BARROS JS, AGUIAR TFM, COSTA SS, et al. Copy number alterations in hepatoblastoma: Literature review and a Brazilian cohort analysis highlight new biological pathways[J]. Front Oncol, 2021, 11: 741526. DOI: 10.3389/fonc.2021.741526. [26] YU WY, LIU X, LI JQ, et al. A single-center retrospective analysis of childhood hepatoblastoma in China[J]. Gland Surg, 2020, 9( 5): 1502- 1512. DOI: 10.21037/gs-20-710. [27] YANG GJ, OUYANG HQ, ZHAO ZY, et al. Discrepancies in neglected tropical diseases burden estimates in China: Comparative study of real-world data and Global Burden of Disease 2021 data(2004-2020)[J]. BMJ, 2025, 388: e080969. DOI: 10.1136/bmj-2024-080969. [28] YUAN LN, TAO JX, WANG JC, et al. Global, regional, national burden of asthma from 1990 to 2021, with projections of incidence to 2050: A systematic analysis of the global burden of disease study 2021[J]. EClinicalMedicine, 2025, 80: 103051. DOI: 10.1016/j.eclinm.2024.103051. -

 本文二维码
本文二维码
计量
- 文章访问数: 351
- HTML全文浏览量: 159
- PDF下载量: 88
- 被引次数: 0

